occupational health service
advertisement

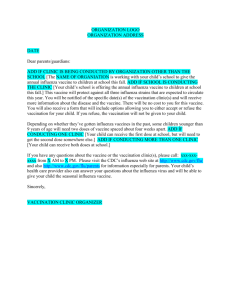
OCCUPATIONAL HEALTH SERVICE Seasonal Influenza Immunisation Consent Form 2010 PRIVATE & CONFIDENTIAL SECTION A Office use only Input date & intls Personal Details Surname: Forename(s): Date of Birth: Telephone number: Occupation: Location: Address: Employer: Please tick NHSG Aberdeen Council Aberdeenshire Council Moray Council B.T.S S.A.S Other G.P.Med. Practice Address: Please answer the following question and mark either the ‘Yes’ or ‘No’ with an X, giving details where required SECTION B Medical Details Yes 1. Do you take tablets/medicine for any reason? 2. Are you allergic to anything - food (e.g. eggs), drugs, animals etc? 3. Do you suffer from asthma or hay fever? 4. Do you suffer from a chronic or recurring illness? 5. Are you or do you think you may be pregnant? 6. Are you breast feeding at present? 7. 8. 9. No Dates & Details Have you had any severe reactions to previous vaccines e.g. rash, tongue swelling, shortness of breath? Have you had any other immunisations or vaccinations during the last six weeks? In the event you suffer an anaphylactic reaction following immunisation you agree to the administration of adrenaline IM as per NHS guidelines. I have read the Influenza Information Leaflet and had the procedure and its implications explained to me. The above information is correct and I consent to having Influenza Vaccine. SIGNATURE: DATE: OHS Nurse / Advisor: I have explained the procedure and administered the following vaccine: Date Vaccine Dose Route Expiry SIGNATURE: PRINT NAME: DATE: Batch