PULMONARY NODULES
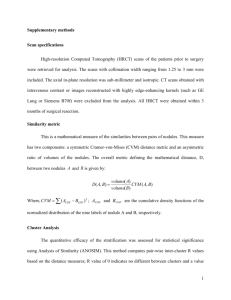
advertisement

PULMONARY BOARD REVIEW: PULMONARY NODULES 1. Multiple Pulmonary Nodules: some etiologies according to immune status a. Immunocompetent 1) Neoplasm - The unexpected discovery of multiple pulmonary nodules in the absence of explanatory elements in the history or on physical examination should raise concern for metastatic malignancy. The most common malignancies to present in this fashion include primary neoplasms of the testes, ovaries, kidneys, breast, and anal canal, as well as melanomas and sarcomas 2) Infection: Bacterial (septic emboli), Viral, Fungal, MTB, MAI, Parasite (hydatid cyst) 3) CVD: Wegeners, RA, Churgg Strauss 4) AVMs 5) Inflammatory Disorder: COP, IIP (RBILD, DIP, LIP) 6) Granulomas: Sarcoidosis 7) Pneumoconiosis: Beryllium, Silicosis, Talc b. HIV: 1) Bacterial PNA 2) MTB 3) KS 4) Lymphoma 5) MAI 6) Lung Cancer 7) Aspergillus c. Lung Transplant: 1) PTLD 2) Aspergillus 3) CMV 4) B.O. 5) Carcinoma 2. Solitary Pulmonary Nodule: single, radiologically visible lesion that is within and surrounded on all sides by pulmonary parenchyma. It is not associated with other, potentially related pulmonary pathology, such as hilar or mediastinal enlargement or a pleural effusion. The upper limit in size of a "nodule" is arbitrary and is generally considered to be either 3 or 4 cm. Lesions larger than 3 to 4 cm are classified as "masses" and are more likely to be malignant. a. Etiologies: Malignant = ~50%, Benign = ~50% (80% infectious granuloma, 10% hamartoma) 1) Malignant: Primary vs. Metastatic (breast, head/neck, melanoma, renal, sarcoma, colon), Carcinoid 2) Infectious Granuloma (MTB, MAI, Fungus) 3) Benign Neoplasm: Hamartoma, Lipoma, Fibroma 4) AVM 5) Bronchogenic cyst 6) Inflammatory – Wegeners, RA 7) Other – pseudotumor, rounded atelectasis, amyloidoma, hematoma, infarct, intrapulmonary lymph nodes b. Factors influencing probability of Cancer: 1) Size: (a) Lung cancer appears to be rare in nodules < 5 mm in size, and it is safe to repeat the CT at 1 year in these patients (b) ~80-90 percent of solitary nodules larger than 3 cm in diameter are malignant 2) Change in size: nodule that grows at a rate consistent with cancer (doubling time of 30 to 360 days) 3) Number: (a) more than six nodules are thought to indicate inflammatory lung disease (b) Synchronous lung cancers are increasingly recognized as CT screening has become more prevalent, and multifocal bronchoalveolar cell or adenocarcinoma is often the histology, particularly in women who never smoked or quit cigarette smoking many years earlier 4) Density: (a) Nonsolid nodule (previously termed ground-glass opacity) is a density through which aerated lung parenchyma is visible - possess a relatively low risk of cancer (approx. 15%); as their size rises > 1.5 cm, the risk of malignancy, particularly BAC rises (b) Solid nodules are the most common, a lower proportion are cancer. Inflammatory diseases of the lung, particularly tuberculosis (typical and atypical) and mycoses, generally produce solid nodules that can be expected to eventually calcify, permitting their designation as benign. Only approximately 15% of solid nodules < 1 in diameter contain cancer, but as solid nodule size increases, the proportion that is cancer increases. 5) Characteristics: (a) Calcification - Pattern: diffuse homogenous (old granuloma), central, concentric (histoplasmosis), popcorn (hamartoma) benign (b) Edge and contour – speculated malignant 6) Age: Lung cancer is rare before the age of 40 years, but its incidence increases steadily from 40 to 80 years (a) 3 percent in patients between ages 35 and 39 (b) 15 percent between ages 40 and 49 (c) 43 percent between ages 50 and 59 (d) 50 percent or higher at age 60 or above 7) Gender: As cigarette smoking has increased in women, the incidence of lung cancer has risen 8) Tobacco: The incidence of lung cancer directly correlates with the pack-yrs of cigarettes smoked. It appears that the incidence of lung cancer stops increasing after smoking cessation, but it does not drop to the levels of individuals who never smoked. Consequently, it is common to encounter patients with newly diagnosed lung cancer who stopped smoking many yrs or decades earlier 9) Spirometry: There is a statistically significant association between a spirometrically demonstrated obstructive ventilatory impairment and lung cancer 10) Occupational history: Asbestos exposure, after a latency period of 20 to 40 years, predisposes to lung cancer acting synergistically with the risk posed by cigarette smoking. Workers exposed to respirable radioactive gas in the production and disposal of fissionable materials have an increased risk of lung cancer. Uranium miners and individuals working with heavy metals such as cadmium and nickel are known to have an increased lung cancer risk. Individuals with idiopathic pulmonary fibrosis and pneumoconioses probably have an increased risk of acquiring adenocarcinoma or bronchoalveolar cell carcinoma 11) Endemic granulomatous disease: As the nationwide incidence of tuberculosis has declined, except notably in immigrants from endemic areas and in HIV-positive individuals, M tuberculosis has become a less common etiology of pulmonary nodules. When CT screening for lung cancer was performed in the Midwest United States, an area endemic with histoplasmosis, a high false-positive rate was observed c. Diagnostic Technique: 1) Evaluate according to risk factors and CT assessment of growth 2) Algorithm #1: CT assessment of nodule growth by Libby, Henschke Chest 2004 et al. – assess size, density, and risk factors (a) Low Risk Nodules: nodules < 5mm, nonsolid nodules 5-10mm repeat CT in one year (b) Intermediate Risk Nodules: (1) part solid and solid 5-9mm and some > 10mm repeat CT in 6 weeks (consider ABx) (2) consider PET (c) High Risk Nodules by risk factors: Biopsy FNA or VATS (d) Repeat CT in 3 months if benign FNA or if does not change or resolves on 6 week CT (e) If does not change in volume in 6 months small risk malignancy < 10% (f) Fails to change over 2 years benign (g) Summary: non-calcified solid nodule > 5mm repeat CT in 6 weeks (consider ABx) or PET (1) If partial resolution or no growth or negative PET repeat CT 3 months (2) If growth or positive PET biopsy 3) Algorithm #2: see attached Ost et al NEJM 2004 approach - in general, unless the likelihood of lung cancer is low/intermediate or the risk of a surgical procedure is high favor removing by VATS such nodules without a biopsy (FNA). 4) Algorithm #3: for <1 cm nodule – see Guidelines for Management of Small Pulmonary Nodules Detected on CT Scans: A Statement from the Fleischner Society 5) FNA: may give three results – (a) Malignant (b) Specific benign – carcinoid, hamartoma, MTB… (c) Nonspecific benign (inflammation, atypia, hyperplasia, blood, bronchial cells, granuloma) - requires careful following for further growth 6) PET: better if > 1cm, SUV > 3 c/w malignancy 7) Bronchoscopy – limited usefulness if peripheral and <2cm 8) VATS – diagnostic Guidelines for Management of Small Pulmonary Nodules Detected on CT Scans: A Statement from the Fleischner Society. Radiology 2005; 237: 395-400. Patients known to have or suspected of having malignant disease.—Patients with a cancer that may be a cause of lung metastases should be cared for according to the relevant protocol or specific clinical situation. Pertinent factors will include the site, cell type, and stage of the primary tumor and whether early detection of lung metastases will affect care. In this setting, frequent follow-up CT may be indicated. Young patients.—Primary lung cancer is rare in persons under 35 years of age (<1% of all cases), and the risks from radiation exposure are greater than in the older population. Therefore, unless there is a known primary cancer, multiple follow-up CT studies for small incidentally detected nodules should be avoided in young patients. In such cases, a single low-dose follow-up CT scan in 6–12 months should be considered. Patients with unexplained fever.—In certain clinical settings, such as a patient presenting with neutropenic fever, the presence of a nodule may indicate active infection, and short-term imaging follow-up or intervention may be appropriate.