this paper - International Campaign for Justice in Bhopal
advertisement

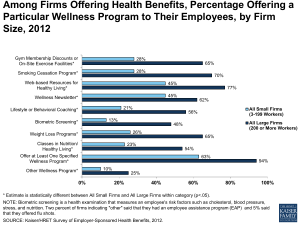
STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION ONE Framing the issue: the Bhopal Gas Tragedy The year 1984 represents a tragic and important milestone in the environmental health arena, particularly with reference to toxic environmental exposure. At around 1AM on December 3rd that year, more than 40 tons of methyl isocyanate (MIC) gas leaked from a pesticide plant owned by the US-based multinational Union Carbide Corporation (UCC) in the small city of Bhopal, India (see maps, Appendix 1). Deadly MIC gas seeped silently across the city, exposing more than half of its population of 900,000, and immediately killing an estimated 3,800 (1). A range of effects has been reported in the aftermath: respiratory, ocular, gastrointestinal, and neurobehavioral disorders were seen immediately (2,3), while in recent years, genetic and reproductive health-related abnormalities have been reported (4-8). The Bhopal Gas Tragedy is the worst industrial disaster of all time. In 1985, as Indian authorities, activists, and survivors navigated uncharted political and legal terrain to hold the US-based Union Carbide accountable, the company’s sister plant located in West Virginia lost over 100 workers in a similar poisoning incident (9). The US response to this domestic incident was expedient: in 1986 the US Emergency Planning and Community Right to Know Act (EPCRA) was passed, giving the public access to extensive data on toxic chemical release and exposure (10). This acted as a gateway for many more hazard safety initiatives related to chemical exposure nationally and internationally (11-13). Yet the success of such safeguards in preventing toxic chemical exposure is questionable: a recent study found that chemical exposure constitutes the highest (28.6%) proportion of exposure incidents from 1996 to 2001 (14) and the National Response Center reports a 25% increase in the number of chemical exposure incidents between 1997 and 2004 (15). PAGE 1 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION ONE This public health analysis is concerned with those affected by or at risk for toxic environmental exposure specifically from the US chemical industry1. This population typically lives near and in most cases concurrently works for the industry. Exposure to environmental toxins in this scenario is affected by an intricate and dynamic combination of determinants. These determinants, furthermore, vary in their relative and cumulative effect across a spectrum of stakeholders, including populations at risk for chemical exposure, chemical corporations, state and national governments, international and UN agencies, and others (discussed later). Social inequality and environmental health determinants Stark differentials exist in access to financial, legal, political, and economic resources between the various stakeholders in this problem. Acknowledging these social inequalities, this analysis adapts Schulz and Northridge’s 2004 conceptual framework of “social determinants of health and environmental health promotion” (see Figure 1, below) (16). The next few paragraphs justify this model of health, describe key determinants comprising it, and indicate the most important one for the target populations in question. Social inequality models for public health have long been researched and advocated for (17-22). They are of special relevance in this context because of the role that the corporate industry – especially chemical multinationals- play in exacerbating health inequalities within and between nations (23-26). Schulz and Northridge’s model sees social inequalities as both resulting in and being a result of disparities in exposure (16)p. 455). Their model depicts a dynamic interplay of fundamental2 (such as natural environment, macrosocial factors, and inequalities), intermediate (such as the built environment and social context), and proximate 1 The chemical industry is the US’ is the world’s largest (responsible for almost a third of the world’s chemicals production), generating over $91 billion dollars a year in export revenue (46). 2 Analogous to, but not synonymous with Link and Phelan’s notion of social conditions as fundamental causes of disease (74) PAGE 2 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION ONE determinants (such as stressors, behaviors, social integration, and social support) that operate through multiple pathways and mechanisms to influence health outcomes. Figure 1 below presents an adapted version of the Schulz and Northridge model guiding this analysis. FIGURE 1. DETERMINANTS OF TOXIC ENVIRONMENTAL EXPOSURE The determinants of toxic environmental exposure are closely related across individual, social/cultural, political, and economic factors and often difficult to distinguish from each other. A better frame of analysis than looking at the determinants separately is considering their relationship to each other. There is global evidence for the differential effect of chemical exposure by gender and age: women and children have worse health outcomes (27-32). This differential effect is not only a function of biology, but also inequalities at other levels involving PAGE 3 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION ONE an interplay of social, economic, and political factors. For example, research on lead exposure in American children reveals the contribution of socio-economic status (social context, intermediate level) and residence in central-city areas (built environment, intermediate level) through putative pathways of immuno-compromized nutrition (health behavior, proximate level) and greater incidence of exposure (stressors, proximate level) (33,34). Consistent with this literature, studies have found that at the intermediate level, enforcing housing policy to prevent lead poisoning and increasing educational and employment opportunities for poor families (both social context, intermediate level) may be effective in reducing lead poisoning rates (16,35). In Cato-Ridge, South Africa, UK-based Thor Chemical’s 1992 mercury exposure incident resulted in three deaths and acute neurobiological morbidity in over two dozen young, poor, black South Africans (36). Here, the lack of industrial monitoring and oversight in government policy at the proximate level had to do with political flux at the end of apartheid, where macrosocial factors such as racism and market pressures at the fundamental level. This resulted in unjust and unequal policy formation and enforcement, creating greater exposure risk and an accountability vacuum (28). These examples and all other evidence point to one key element affecting all determinants: the unequal distribution of power and health. The most important determinant, then, is that which enables public health to redistribute unequal power and health among stakeholders. Industrial Codes at the Intermediate Level: Creating a Public Health bridge for equity As the aforementioned mercury and lead case demonstrate, macrosocial factors are at the root of inequality; they trigger risk along contextual and behavioral factor-driven pathways. As such, they are the most influential. Yet, these determinants are also the most difficult to influence. Interventions at the fundamental level entail changes in political or economic order PAGE 4 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION ONE that are typically beyond the scope of public health. On the other hand, public health interventions have historically focused on reducing effects post-exposure (i.e. at the proximate or outcome level) (5,37-39). These interventions have had limited success because proximate level factors typically cannot prevent exposure incidents from recurring since they do not address the inequalities that perpetuate them. In concurrence with Schulz and Northridge, from whom the current conceptual model derives, this analysis will focus on a determinant at the intermediate level in the social context category: industrial codes (see item in red, Figure 1). Industrial codes related to environmental exposure have been chosen as a significant determinant because they best meet the main criterion of maximizing the redistribution of health and power through public health. This is because industrial codes hold accountable industries and related stakeholders who are usually directly responsible for toxic environmental exposure. Industrial codes affect and are affected by national and international policies across domains (such as occupational and environmental health) and nations, and offer opportunities for multiple stakeholder involvement in the formation, implementation, and revision of industrial practices outside government bureaucracy. They can interact with policy to institutionalize a set of “best” practices” to preserve public health. Finally, and most importantly, with respect to this target population, a code applied to industry is one of only a few tools that can be implemented transnationally, hold multiple parties accountable, and address local and international factors affecting toxic environmental exposure. PAGE 5 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO The Bhopal Aftermath: the need for accountability Industrial codes have been recognized as the most important determinant affecting toxic environmental exposure from the chemical industry. In this regard, the Bhopal Gas Tragedy in 1984 was a watershed event. Insofar as no major policies around exposure to chemical toxins existed prior to this, Bhopal framed most of the world’s major industrial codes as governments, UN agencies, and corporations devised strategies to reduce risk and liability while maximizing accountability and safe operation in chemical industry process management (see summaries of key interventions, Appendix 2). In the global arena, the International Program on Chemical Safety, a joint initiative of the United Nations Environmental Program (UNEP), the International Labor Organization (ILO) and the World Health Organization (WHO), issued two codes of practice as guidelines for industry and government (12). These codes, Prevention of Major Industrial Accidents and Safety in the Use of Chemicals at Work, are nonbinding and have been of little consequence to countries like the US and India, which did not even ratify the related ILO conventions. In the US, where most of the world’s largest chemical corporations are headquartered, the only body creating codes or standards affecting US based industries is the Department of Labor’s Occupational Safety & Health Administration mandated by the Occupational Safety and Health Act (OSHA) of 1970. OSHA went into effect in 1970 to enforce industrial standards ensuring workplace health (40). Even after the poisoning of the West Virginia Union Carbide facility, no additions or amendments related to exposure or facility management were made to the 1970 standards of permissible chemical exposure levels for workers. As recently as 2002, the OSHA administration was still enforcing the 1970 standards; its 1991 effort to update standards was overturned by federal courts (41). The current administration has shelved over a dozen OSHA PAGE 6 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO initiatives to update standards (42,43). Responsible Care®: the chemical industry codifies itself In the midst of these activities (or lack thereof), the multinational corporate sector crafted its own industrial code of practices related to toxic environmental exposure. Immediately pursuant to the Bhopal disaster, in 1985, the Canadian Chemical Producers’ Association (CCPA) launched its own voluntary code of conduct, Responsible Care®3 (44). Chemical corporations and associations in 46 additional countries have since followed suit, on US foot-heels (44). Responsible Care® in the United States Responsible Care® was adopted in 1988 by the US Chemical Manufacturer’s Association (CMA, renamed the American Chemistry Council, ACC in 2000). The aims of the program are to improve chemical processes, significantly reduce waste, minimize accidents, safely produce, transport, use and dispose of materials, enhance customer relations and service, and increase communication with the public (45). The Responsible Care® program has amended and adapted its requirements over the past 17 years; currently, constituent chemical industry firms, as a condition of their ACC membership, adopt the following: 1. Ten guiding principles that are agreed upon by all ACC member firms (see Appendix 3) (46); 2. A Responsible Care Management System (which in 2002 replaced the previously upheld codes of conduct) and related Security Code (see Table 1, below) (47): 3 Interestingly, one of the first companies to endorse Responsible Care® was Dow-Canada (50), whose parent company acquired the now infamous Union Carbide in 2001 (75). In addition, it is reported that the US chemical industry adopted Responsible Care® upon the initial suggestion of Union Carbide’s Chief Executive Officer, Robert D. Kennedy, (50) suggesting important linkages between Dow Corporation, Union Carbide Corporation, and Responsible Care®. PAGE 7 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO TABLE 1: RESPONSIBLE CARE® MANAGEMENT SYSTEM AND SECURITY CODE ELEMENTS (47) 1. Leadership Commitment. Senior leadership commitment to continuous improvement through published policies, provision of sufficient and qualified resources and established accountability. 2. Analysis of Threats, Vulnerabilities and Consequences. Prioritization and periodic analysis of potential security threats, vulnerabilities and consequences using accepted methodologies (i.e. those developed by Sandia National Laboratories, the Center for Chemical Process Safety or equivalent methods). 3. Implementation of Security Measures. Development, implementation, and documentation of site, cyber and transportation security measures commensurate with risks, taking into account inherently safer process design, engineering and administrative controls, and prevention and mitigation measures 4. Training, Drills, and Guidance. Training, drills and guidance for employees, contractors, service providers, value chain partners and others, as appropriate, to enhance awareness and capability. 5. Communications, Dialogue, and Information Exchange. Communications, dialogue and information on appropriate security issues with stakeholders such as employees, contractors, communities, customers, suppliers, service providers, and government officials and agencies balanced with safeguards for sensitive information. 6. Response to Security Threats/Incidents. Evaluation, response, reporting, communication and corrective action in response to threats and/or incidents. 7. Audits and Third-Party Verification. Audits to assess security program implementation and third party verification at facilities with potential off-site impacts to ensure physical security. 8. Management of Change and Continuous Improvement. Evaluation and management of security issues associated with changes involving people, processes, products, information or information systems. Continuous improvement of performance, process planning, establishment of goals and objectives, monitoring, analysis of trends, and the development and implementation of corrective action. 3. A battery of industry-wide Performance Measures across a broad range of issues including economics, environment, health, safety, and security (see Appendix 4), to be made available to the public (This is a recent addition, the reporting requirement for most of these measures begins this year) (46); 4. Public Dialogue through Community Advisory Panels (CAPs) is required, where community members, environmentalists, civic, business and education leaders, as well as health and safety specialists may meet with the management at any facility to discuss issues of mutual interest (46). 5. Membership in Responsible Care® is open to partner associations and companies who are not members of the ACC (46). These groups follow the protocol of the ACC as PAGE 8 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO members, including payment of fees and accountability to protocol (48) but are not included in official reporting to the Responsible Care® international governing body (49). Why the US Responsible Care® Program is a good case study The most important determinant affecting toxic environmental exposure is industrial codes governing toxin exposure. Chemical corporations have direct control over exposure and as such, standards that apply directly to them are most relevant. Responsible Care® is maintained by and applies to the ACC, which comprises 191 of the biggest chemical firms based in the US, including large multinational corporations (MNCs) like Dow Chemical, DuPont, and Bayer. In addition, it is also important to note that this program was developed in direct relationship to the Bhopal disaster, which is the frame not only of this, but most analyses of toxic exposure and the chemical industry. Furthermore, unlike OSHA or the ILO conventions, Responsible Care® is one of the few (if any) interventions that apply to multinational corporations and their subsidiaries. As the following sections reveal, furthermore, this intervention reveals and affects the critical health and power inequality dimensions underlying the most important determinant related to toxic environmental exposure. Given these connections and because of the wideranging implications US industry standards have in today’s globalizing world, the American Responsible Care® program is an important case-study. Is Responsible Care® Appropriate? Appropriateness is considered here in terms of timeliness, relevance to the population of interest, involvement of key stakeholders in policy development, and consideration of ethical issues. The adoption of Responsible Care® in the US took place four years after the biggest industrial disaster in the world. A precursor to the community awareness component of the PAGE 9 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO program was implemented as early as 1985 (50), and as such, reflected the urgent desire of the chemical industry to improve its environmental health and safety standards (and, in tandem, its public image after the Bhopal catastrophe). Furthermore, as per item five of the code and component four of the program, the chemical industry is required to have public dialogue through CAPs which is an opportunity to engage key stakeholders and bridge the health and power inequalities mentioned in response to Question One. Yet, no mechanism exists to incorporate the conclusions or findings from public dialogue into the implementation of Responsible Care®. In addition the caveat “safeguards for sensitive information” may be used as a loophole for nondisclosure of issues that may be important to the public. The notion of the chemical industry voluntarily codifying itself at its own pace without penalty has a lot of practical problems, particularly related to accountability. De facto, the industry is accountable to itself, which is ethically very weak, particularly from the perspective of those at risk for poisoning. Indeed, Responsible Care® doesn’t necessarily ensure that a situation like Bhopal won’t recur (the protracted legal battle around the 1984 gas leak is itself ongoing in spite of this program, and incidents of toxic chemical exposure have only increased (51). Thus, one must conclude that Responsible Care® is limited in its appropriateness. Is Responsible Care® Effective? Effectiveness is defined as the degree to which a program meets its aims and how well it improves the health condition of those at risk of toxic environmental exposure. To begin with, data for international populations could not be found. This could either be because it has not been made public, or that it is not gathered in the first place. Either scenario reflects poorly on Responsible Care® and violates its aims of increasing communication with the public. Future analysis uses domestic data with the assumption that international figures will likely be less PAGE 10 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO favorable given the more lax industrial standards in most developing nations. A major issue with respect to the effectiveness of Responsible Care® is that the frequency and process of monitoring and evaluation is in large part governed by the ACC. The only penalty for noncompliance, furthermore, is peer disclosure (i.e. other firms are made aware of your noncompliance). King and Lenox’s 2000 study concluded that membership in Responsible Care® was not associated with reductions in toxic release as compared to nonmembers (52), which violates multiple aims of this program (this will be discussed further in response to Question Four). Moreover, the US Public Interest Research Group (PIRG) found that 75% of the facilities were either not willing or unable to share information about chemical risk required by the Communication, Dialogue and Information Exchange provision of Responsible Care® (51). This and other examples discussed in response to Question Three suggest that Responsible Care® lacks effectiveness. Is Responsible Care® Comprehensive? Comprehensiveness refers to the breadth, depth, and interrelatedness of program components. On paper, this program appears to cover many bases, from involving stakeholders to monitoring and amending security mechanisms. As such, this set of standards has the potential to affect multiple determinants: it can bring about social justice and corporate responsibility on the macrosocial/fundamental level, increase civic participation and community investment at the intermediate level, and reduce stressors at the proximate level. Yet, even on paper, some of the program components (such as public dialogue) are given tokenistic attention, raising doubts about the actual comprehensiveness of the program. Moreover, Responsible Care® allows firms to adopt components of the code at their own pace (53). This is presented as an incentive inasmuch as gradual adoption reduces the up front costs of membership in the PAGE 11 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION TWO program. Yet this feature renders Responsible Care® vulnerable to opportunism and moral hazard, where firms join the program, and while delaying its implementation, take advantage of the benefits it affords (mostly reputational). Furthermore, piecemeal adoption of the program reduces its comprehensiveness for firms and stakeholders. On the industry level as well, variations in adoption between firms compromises the comprehensiveness of Responsible Care® overall. The following pages lay out these inconsistencies between firms as well as between the potential and actual use of the Responsible Care® standards. PAGE 12 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION THREE The Walt Policy Framework: actors, context, processes A useful analytic tool in discussing the financial, implementation and feasibility-related aspects of Responsible Care® is Walt’s policy framework for international public health, which focuses on “the role of actors, and how they are affected by, and influence, the context and processes within which policies are made and implemented”(54). Responsible Care® is not international policy in its strictest sense. Yet, Walt’s framework applies because the program is a code guiding processes with transnational implications that have been strongly influenced by the actors involved in the chemical industry in a specific historical context. In discussing the financing, implementation and feasibility of Responsible Care®, this analysis will refer to actors, contexts and processes to demonstrate the relationship between program rhetoric and reality. Financing The financing aspects of Responsible Care® have not been made public. Yet, some conclusions and estimates can be made from internal ACC documentation acquired by the Chemical Industry Archives on the basis of Freedom of Information Act requests to the government (48). Responsible Care® activities are funded by annual fees paid by member companies as a percentage of their annual chemical sales (the calculation rubric is not publicly available) and flat fees assessed upon partner firms and associations (48). While it is unclear whether fees assessed upon partner associations and firms are comparable to member fees, internal documents collected by the Chemical Industry Archives reveal annual partner member fees of 82,400 USD and higher in 1991 (48). Some transportation and insurance firms have offered economic benefits and incentives to chemical companies who adopt Responsible Care® (50), yet small firms in the chemical industry are reluctant to adopt it. Prakash explains: “Responsible Care® is a project of large chemical firms that can afford to create specialized structures and employ personnel…in PAGE 13 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION THREE contrast, the organizational structures of smaller firms typically reflect little functional differentiation…there are fewer procedures and relatively less documentation of management systems” (50). Thus, Responsible Care® is necessarily adopted only by those who can afford it. The implementation and operational costs of Responsible Care® in each facility are borne by individual firms. From 1990 to 1996, the ACC (then CMA) spent between 1-2 million USD per year on implementing Responsible Care® in member companies, and about 8.5 million USD on advertising as part of a public outreach campaign to improve the public image of the chemical industry (48). The 1984 Bhopal Gas Tragedy and the 1989 Exxon Valdez spill provide context to this skewed allocation of resources: the chemical industry had a very poor reputation at this point. Their process: greater fiscal emphasis on ameliorating the chemical industry’s public image (a 4% increase was seen in favorable public opinion in 1995 (50)) than on improving its safety procedure and operations. From the perspective of the chemical industry, this is cost-effective; this opinion is not shared by other actors and stakeholders (labor unions, community members, and environmental experts) (48,51,55). Unfortunately, these groups are often excluded from the implementation process and only involved at the outcome level (when exposures occur). Implementation At the outset, the structure of the US chemical industry explains the origins and current implementation of Responsible Care®. The industry is oligopolistic, with a small number of very large firms dominating the industry’s practice (56). These large firms internalize a large portion of the collective reputation of the industry (57), and in response, initiate the establishment of industry standards and codes. This is especially true in the environmental health arena (58). The voluntary and self-regulatory nature of Responsible Care® allows the hegemons within these oligopolies to pursue their self-interest on their own terms (50), and PAGE 14 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION THREE create benefits for others in the process. These factors explain the chemical industry’s deliberate central role as an actor, which in turn creates a context of diffusion and staggered implementation of Responsible Care®. To begin with, Responsible Care® charges chemical companies themselves to plan, implement, and update its components. The only time when companies may not completely drive the process is in the monitoring phase of implementation, that too, at firms’ own discretion. One such opportunity arises in the form of Citizen Advisory Panels that generate feedback on public perceptions and concerns. While there is evidence for CAPs changing facility practices (59-61), studies also suggest that CAP participants tend to be very similar to facility managers in most sites and rarely comprise environmental advocates (62). Since the selection of CAP members is the prerogative of firms themselves, it appears that many firms are deliberately losing the richness and relevance of feedback and information that could be obtained from a broader selection of CAP members. More likely than not, stakeholders (such as at-risk populations) with opinions that are unpopular with facility managers are purposely not represented in CAPs and consequently play no role in the implementation of Responsible Care®. Additionally, firms have the discretion to choose peer auditors to verify whether or not management systems are in place (63). Stronger, more public and participatory monitoring mechanisms exist, such as those conducted by the public or third parties (this latter option is required for the ISO 14001, another industrial environmental health and safety code) (11). Yet, the ACC has deliberately chosen not to administer these methods of verification for Responsible Care®, losing the value addition of external expertise and approval. Another weakness is that while auditors verify the presence of a management system, firms conduct system performance evaluations themselves (it must be noted that performance evaluation standards were only added in 2002; the first round of reporting for most measures began last year, see Appendix 4). PAGE 15 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION THREE Evaluating performance is a key area where the involvement of stakeholders could improve health outcomes. Responsible Care® does not enable this. Another weakness of implementation is that the highest sanction for incomplete adoption of Responsible Care® is peer disclosure. This is a weak sanction; a stronger sanction would be public disclosure of company compliance to safety standards, which would allow the public to place pressure upon and thus increase stakeholder involvement with Responsible Care®. Nash describes the placement of Responsible Care® in a diffusion model of strong and weak sanctions and monitoring (see Appendix 5). Responsible Care® is located at the center of the matrix, which is characterized by an accountability vacuum (63). It is no surprise, then, that practices across US firms are inconsistent. A 1995 study found substantial variations –a diffusion –in the adoption of Responsible Care®, as per the following typology in Table 2: TABLE 2. HOWARD AND COLLEAGUES’ LEVELS OF RESPONSIBLE CARE® IMPLEMENTATION (62) 1. Drifters were companies that said Responsible Care® had little impact on their activities. Changes were limited to documenting existing practices. 2. Promoters used Responsible Care® mainly to promote a strong environmental reputation to external stakeholders, and Responsible Care as “formalizing” and “standardizing” what they already did. 3. Adopters saw Responsible Care® as a valuable tool for improving their environmental practices and had introduced new practices in community relations and distribution 4. Leaders spoke about Responsible Care being a “whole new way of thinking;” that whereas their environment, health, and safety (EHS) practices were strong before Responsible Care, the initiative offered a way to progress The above trend in the adoption of Responsible Care® reflects the Rogers’ model of Diffusion of Innovations (64) that the EPA reports is typical in environmental health management (65). Inasmuch as Responsible Care® is self-regulated, however, it is unclear whether the firms in each category will remain in their positions, or if pressure from the latter categories will cause a shift to more concerted implementation of the program, as theorists suggest (66). Finding and predicting trends is difficult since variability exists both within and between firms. Nash concludes: “firms adopt Responsible Care® in their own way, at their own PAGE 16 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION THREE pace, and results in terms of environmental performance vary substantially” (63). Feasibility The implementation of Responsible Care® across the industry is inconsistent and its effectiveness in meeting public health targets, questionable (this is discussed in responses to Question Two and Four). Yet for the ACC, Responsible Care® is cost-effective, sustainable, and feasible: it has lasted over 17 years. Questions of feasibility arise when other stakeholders, the global context, and alternatives to Responsible Care® are considered. The international coordinating body for Responsible Care®, the International Council of Chemical Associations (ICCA) admits in its 2002 report that it has been “slow to recognize the need for, and implementation of, effective partnerships with critics” (49). Potential critics have been excluded from the CAP process in the US (62) and inasmuch as many of these critics reflect the concerns of stakeholders most vulnerable to toxic chemical exposure, the chemical industry is making itself vulnerable to great criticism should another event like Bhopal recur. The ACC scaled up its engagement with state and federal government stakeholders and created a Security Code in 2002 in the midst of rising political concerns over the risk of chemical exposure from terrorist attacks after 9/11, (47). Yet, taking a closer look at the Security Code, one sees almost complete overlap with the previous Responsible Care® management system (so much so that they are presented together in this analysis). Unfortunately, from Bhopal to 9/11, it appears that the main motivation for ACC to involve more stakeholders or amend Responsible Care® is when a disaster has occurred or when the threat of one is highly politicized. On the global scale, meanwhile, the ACC has jeopardized broader implementation and endorsement of Responsible Care®. In 2001, efforts to reach a global agreement on Responsible Care® with the International Federation of Chemical, Energy, Mine and General Workers’ Unions (ICEM) were thwarted by the ACC, apparently at the behest of ACC members Exxon PAGE 17 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION THREE and DuPont (55). A global agreement would have set the stage for international cooperation, monitoring, and endorsement by a wider spectrum of stakeholders (beyond ICEM). More importantly, setting uniform international standards for occupational and environmental health and safety would directly address the inequalities and inadequacies that caused the Bhopal Gas Tragedy in the first place. The ACC’s actions have soured its relations with other national chemical associations and may have long-term effects on the American chemical industry and Responsible Care®. Interestingly, there are few if any major differences between the Responsible Care® guidelines and alternatives (for a list, see Appendix 2). This is because in most cases, Responsible Care® incorporates these standards in its own framework (48). This strategy allows Responsible Care® be at par with existing standards, but enforce them more loosely. Yet, in the long run, this may cost Responsible Care® its popularity in the chemical industry, particularly as non self-regulated codes become more commonplace worldwide. PAGE 18 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE Evaluations of Responsible Care® No official or ACC-endorsed evaluations of the Responsible Care® program exist. Instead, the ACC has posted some statistics on environmental health standards on the US Responsible Care® website (www.responsiblecare-usa.com), based on member company reports. A useful theoretical assessment of the program was carried out by Prakash using various economic theories to discuss Responsible Care’s® voluntary nature (50). The National Public Interest Research Group, a nonprofit watchdog, conducted original research and published two reports: one in 1998 based on interviews of facility staff from ACC member firms and the second in 2004 based on chemical incident reports to the National Response Center (51,67). While the latter of these is the most recent evaluation of Responsible Care® and shows interesting trends across time, location and by company, the relationship between these elements and other variables is not explored. It is a descriptive study and lacks the richness that befits a more thorough evaluation of Responsible Care®. Nash teamed with Ehrenfeld to compare Responsible Care to other industrial codes in the United States (42) and with Lenox to compare codes across industries (68). However, given the previous discussion on the implementation and feasibility of Responsible care, the most appropriate evaluation is King and Lenox’s 2000 study looking at predictors of membership as well as a case control comparison of environmental performance (52). The King and Lenox evaluation: purpose, process and design As mentioned earlier, the aims of Responsible Care® are to improve chemical processes, significantly reduce waste, minimize accidents, safely produce, transport, use and dispose of materials, enhance customer relations and service, and increase communication with the public (45). King and Lenox’s 2000 study evaluates the first four of these aims. Its purpose was to determine whether industrial self-regulation within for-profit industries can be effective, looking PAGE 19 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE specifically at the characteristics of Responsible Care® formation and membership, as well as members’ environmental performance and improvement of relative to nonmembers in the industry (52). These researchers’ work was supported by the Massachusetts Institute of Technology (MIT) Business and Environment Program and carried out by researchers on MIT and New York University premises. Data was collected from the Environmental Protection Agency’s (EPA) Toxics Release Inventory (TRI)4 which has collected facility-level reports of the emissions of over 200 toxic chemicals from US manufacturing firms from 1987 onwards. While the researchers do not indicate their sampling strategy, it appears that all observations within the chemical industry in this inventory were used, comprising 22,476 observations from 3,606 facilities and 12,829 observations from 3,606 firms in the period 1987 -96. Of this group, Responsible Care® membership was determined for all firms in the period 1990-6, and CMA membership in the three years prior (1990 was chosen as base year because Responsible Care® was ratified by the industry in October 1989). Researchers found that Responsible Care® firms, due to their size, accounted for as high as one-third of the facilities reported in the TRI in a given year. Table 3 below outlines the variables used in this study, and their measurement. TABLE 3. VARIABLES AND MEASUREMENT IN KING AND LENOX (2000) VARIABLE MEASUREMENT CMA Membership/ Using data from the CMA firms and facilities were binary coded (yes/no) for each year (1987Responsible Care® 96) Participation Environmental (Weighted) emissions were calculated using yearly averages of pounds of emission for Performance, facilities with weights for production in each facility as a proportion of its parent firm’s Relative and Sector productivity, and emission toxicity (as per EPA standards). Relative Emissions at the facility level were calculated (using ordinary least squares regression) as the deviation between observed and predicted emissions given facility size and sector. Sector Emissions at the firm level were calculated in groups based upon Standard Industrial Classification (SIC) codes, which codify sectors by the level of hazardous emissions. 4 The TRI was created in 1986 in direct response to the Bhopal Gas Tragedy as part of the Emergency Planning Community-Right-to-Know Act (see response to Question One). As per this Act, businesses are required to report chemicals release to the TRI for each facility on an annual basis (10). PAGE 20 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE VARIABLE Environmental Improvement, Absolute and Relative Organization Size Focus within the chemical industry Firm visibility MEASUREMENT (Researchers refer to these in their analysis as more or less dirty firms.) Absolute improvement was measured as the percent change in total weighted emissions over one year Relative improvement measured the percent change in relative emissions (see above) over one year Size was measured as a log of the sum of all employees at all of the firms facilities using Dun & Bradstreet Focus was measured as the log of the total number of employees in the chemical industry over the log of the number of employees in the company (this variable grew with the degree to which a company was focused on chemicals) Visibility was measured as a continuous variable varying from 0 to 1 based on a random sample survey of students (n=25-35) at the NYU Stern School of Business. Visibility was determined as the percentage of students who recognized a company’s name and/or brand out of the number who were asked to respond for that company. King and Lenox used these eight measures to test five hypotheses related to Responsible Care® membership, environmental performance and improvement. The researchers’ hypotheses analytical strategy, and findings are presented in Table 4 below: TABLE 4. HYPOTHESES, ANALYTICAL STRATEGY, AND FINDINGS FROM KING AND LENOX (2000) HYPOTHESIS ANALYTICAL STRATEGY SIGNIFICANT FINDINGS (P<0.001) 1: Firms are more likely to A probit model was used; the likelihood Larger firms, those firms whose business be members of the CMA that a given firm within the chemical was focused in chemicals, and more visible and participate in industry will be a CMA/Responsible companies were more likely to be Responsible Care® if they Care® member was the dependent CMA/Responsible Care® members. In are larger, more focused in variable; independent variables were 1990, the likelihoods of membership were chemicals and have high relative emissions, focus, visibility, and 24%, 47% and 124% higher for these visibility size. Three models were devised for (a) groups, respectively. Of particular interest is the membership in 1990, (b) entrants in the strong “visibility” effect. 1991-6, and (c) exiters in 1991-6 There were no significant differences between firms who joined Responsible Care® and firms who left it from 1990-96 2: Firms are more likely to The probit model above was used Companies with weaker environmental be members of the CMA performance relative to their sectors (the and participate in relative emissions variable) and higher Responsible Care® when sector emissions (i.e. companies that are they have higher levels of dirtier) were more likely to be pollution relative to their CMA/Responsible Care® members. In industries, operate in 1990, higher relative emissions firms were industry sectors with 24% more likely and higher sector emissions higher average levels of firms were 45% more likely to be members pollution 3: On average, firms that A generalized least squares regression Models explain only 5-7% of the variance. participate in Responsible model was used with White’s correction Data provide no evidence that the rate of Care® will improve their for heteroskadasticity (increasing environmental improvement is higher in environmental variance with size of variable) and a members. In fact, members were found to PAGE 21 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE HYPOTHESIS performance more than nonmembers in the industry 4: On average, the chemical industry will more rapidly improve environmental performance after the inception of Responsible Care® 5: In direct contrast to Hypothesis 3, on average, participants in Responsible Care® will improve their environmental performance less than nonmembers in the industry ANALYTICAL STRATEGY fixed-effects specification (where, in longitudinal data sets, unobserved heterogeneity can result in incorrect inferences about the significance of individual effects) and robust specification to control for nonnormal data. Absolute and relative environmental improvement were the dependent variables; the independent variables were membership, relative emissions, sector emissions, focus, visibility, and size. Estimates were calculated at the firm and facility level A similar generalized least squares regression model was used with an interaction term for two time dummy variables, the 1987-89 period and 199096 period. Absolute rates of improvement were the dependent variable; the independent variables were membership, time, sector emissions, focus, visibility, and size The model for hypothesis 3 was used SIGNIFICANT FINDINGS (P<0.001) be improving up to 5% slower in comparison to nonmembers (although this may attributable to low turnover in Responsible Care® membership) Models explain only 2-3% of the variance. The rate of improvement in the entire chemical industry increased around 12 % firm wide and 19% at the facility level after the inception of Responsible Care®. However, the rates of improvement in member firms and facilities were lower (9%) overall and did not significantly chance after 1990. Researchers suggest this may have been because nonmembers, because of their non-adoption of Responsible Care®, were under increased pressure and scrutiny and improved environmental performance more rapidly Models explain only 5-7% of the variance. In tandem with Responsible Care® members’ slower relative environmental performance compared to nonmembers, their absolute environmental performance is lower, though not significantly. In summary, this evaluation of Responsible Care® found that members typically comprise large, highly polluting, and highly visible firms who have improved environmental performance slower (and less) than their nonmember peers through 1996. Strengths and Weaknesses in Design, Measurement, and Conclusions King and Lenox’s study design has high face validity because it contextualizes Responsible Care’s® relationship to chemical exposure by looking at factors related to PAGE 22 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE membership, firm design and focus. The use of the EPA TRI database shows good criterion validity because it looks at exposure and emissions data and is discriminant from accident data used in other evaluations (51). (Chemical exposure can have long ranging effects that are often not recognized or reported as accidents.) The established EPA measure of toxicity was preferred by researchers over the newer, less validated scale developed at Purdue, showing attention to validity and reliability issues. This evaluation has good explanatory power as a result. The researchers show innovation and expertise in measurement design, using weighted scales for emissions, gathering data across firms and facilities, undertaking a mini-survey project to determine the variable for visibility, and applying a case-control analysis on longitudinal data. The strength of design is that all emissions data are used (randomization is not necessary!) and while the research is unobtrusive and observational, a pre-test post-test control group design is used (observations comparing member and nonmember firms from before and after the ratification/widespread adoption of Responsible Care®). Most threats to internal and external validity such as selection, instrumentation, attrition, and the interaction of treatment with selection are thus bypassed. Notwithstanding, King and Lenox’s study has some limitations. Researchers admit that they were unable to completely control for differences between facilities, which may vary greatly within and across companies based on factors not included in the model, such as type, age and location of facility. Another major limitation is the possibility that the greater number of emissions observed for Responsible Care® members is actually a result of more diligent reporting as required by the code itself. Researchers devised the improvement variable to capture such differences, yet if reporting became more stringent as time went by, this is likely to offset improvements in environmental performance for member companies. This is an external validity threat where testing and treatment interact. Finally, King and Lenox point out that the industry PAGE 23 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE reduced emissions by nearly 50% in this period, which may or may not be attributable to Responsible Care®. Indeed, at this time, the government sponsored 33/50 industrial code was in place, requiring firms to reduce emissions by 50% by the year 1995(11): this is a clear case of multiple treatment effect. Beyond what the researchers report, an important limitation of the study is its outdatedness (data from 1987-96). Responsible Care® has undergone some significant changes from 2000 onwards, such as the changing of CMA’s name to the ACC, a performance reporting requirement and third-party systems verification option, which are specifically crafted to improve management for better environmental performance and increase public approval. The changing nature of the treatment creates an external validity threat and limits study generalizability. Furthermore, the models used for Hypotheses 3-5 in this study have very low regression coefficients, suggesting that many other factors not addressed here (such as location, state and federal policies- the 33/50 program- and perhaps CAP involvement) affect environmental performance. In addition, the frame of yearly improvement in environmental emissions may not reflect program effect inasmuch as codes and standards may take longer to affect environmental performance. An absolute change measure across the five-year period may reveal such trends. Differences between firms could also be analyzed more specifically by collecting quantitative data using Howard and colleagues typology (see Table 2, (62)). This evaluation of the Responsible Care® is very telling and despite limitations, important conclusions can be drawn from it, not the least of which is the following: The chemical industry affects a physical commons – clean water, clean air, and health ecosystems – but it was not the threat that this shared public good that motivated the industry’s initial attempts at self-organization. Rather it was a threat to a second, reputational commons that sparked the creation of Responsible Care (52). PAGE 24 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE The reputational commons motivation behind this self-regulated industrial code has wideranging implications for future research, intervention design, and policy development around toxic environmental exposure. The following section explores future directions in these areas. PAGE 25 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE Responsible Care®: whose health? The most important determinant with respect to toxic chemical exposure from industry is industrial codes of conduct. Inasmuch as Responsible Care® is the oldest and largest industrial code in the chemical industry (see Appendix 2) it is at the center of this analysis. However, as this analysis has shown, Responsible Care® has thus far failed to meet its own aims and had little impact on improving environmental health outcomes and reducing risk. It has, however, succeeded in improving the public image of the chemical industry after a series of accidents in the 1980s (11,48,50,52). So, whose health does Responsible Care® protect and why? It seems as though most of the provisions of this code ensure the economic and social health of companies rather than the health of communities at risk of toxic exposure from their activities. King and Lenox describe this ethos of having the “reputational commons” (see quote in response to Question Four) be the operative goal driving the formation of Responsible Care, at the expense of the ACC’s publicly touted “physical commons” goal (52). In the era of globalization, where market profit is the bottom line, it is perhaps naïve to think that an industrial self-regulating code would operate differently from how Responsible Care® has. This combined with the US ethic of individualism explains the way in which the ACC has operated. Given this ethic and a market profit motive, the ACC, holding its own interests above all others, has chosen to self-regulate in order to maximize control over its processes and deflect regulation. Inasmuch as those affected by and at risk for toxic chemical exposure are poorly represented in the ACC, they neither control the code nor the operative goals that guide it. The unfortunate consequence is that Responsible Care® maintains the health and power inequalities industrial codes otherwise have the potential to reduce (described in response to Question One). Thus, the issue here is not that industrial codes are a poor determinant of environmental health but rather that certain qualities of Responsible Care® (its voluntary nature, PAGE 26 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE lack of sanctions and rigorous monitoring, and premise of self-regulation) render it an inefficient strategy in addressing this determinant. This analysis explores other aspects of Responsible Care® that might make it more capable of addressing the problem, such as research, additional components/ interventions, and/or policy. Furthermore, there are research, intervention and policy strategies outside the scope of Responsible Care® that may prove also useful in addressing the public health problem. The most appropriate of these is discussed in conclusion. Making Responsible Care® more responsible: research, intervention and policy directions As explained in response to Question Two, surveys of Responsible Care® member firms show a diffusion of adoption (62). Studying the proportions and characteristics of this diffusion may help the ACC devise strategies to increase and equalize membership and compliance. The biggest gap in research, however, is regarding the adoption and implementation of Responsible Care® internationally. While Responsible Care® standards apply for all facilities, no data from outside the United States is reported on the Responsible Care® website. Some firms such as Dow and Bayer indicate that they follow Responsible Care® standards (69,70), but data on their environmental performance is not available for all countries. Researchers outside the industry in the fields of environmental and occupational health, industrial management and policy, and international development and globalization studies have not looked at this either. As firms increasingly outsource production and manufacturing to the developing world, this research trajectory will be very important in monitoring the environmental effects of Responsible Care®. The issue of monitoring is a contentious one with respect to Responsible Care®. In the US, third parties from the industry are involved on a discretionary basis in monitoring American companies. In Canada, Responsible Care® is verified by four-person teams which are wholly independent of the company, composed of ordinary citizens, industry members, environmentalists and academics (11). Over several days, each team goes on plant tours, PAGE 27 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE conducts extensive interviews, examines company documents and makes calls to neighbors, customers and suppliers. Team members then write a detailed report, and the company shares the results of that report with employees, neighbors and peers. It seems that in Canada, the reputational commons and physical commons are perceived as being far closer together, such that the industry is willing to divest some regulatory power to third parties potentially affected by its activities to improve its public image. This logic and monitoring method may be worth pilot testing in the United States as a small-scale intervention, though strong industry resistance to this idea would have to first be overcome. Another intervention that could be tested with relation to Responsible Care® is the use of harsher sanctions. Currently, noncompliance in the adoption of Responsible Care® components is sanctioned by peer disclosure. Public disclosure (which has worked well in Canada (11)) or some kind of mandatory fine mutually agreed upon by the ACC may raise accountability and compliance in the industry. Here, one could rely on the lobbying efforts of subsidiaries of large multinationals that operate in countries with more stringent Responsible Care® regimes. For instance Dow-Canada could encourage or incentivize its US partner to advocate public disclosure or fines in the US setting. Given the size and influence of this corporation, it is likely that if Dow-US pushes for sanctions, the ACC will be able to get more companies on board. On the policy level, Responsible Care® could really benefit from more stringent government control over the industry. As mentioned earlier, the post 9/11 emphasis on chemical security in case of terrorist attack has resulted in the adoption of the security code element in Responsible Care®. Yet this code comprises no new elements. This undermines the heavy reliance of chemical security on a company’s environmental and health standards and the need for more stringent controls, especially in the event of a terrorist attack. Strategically, federal and state governments could use the frame of chemical security to legislate more stringent oversight PAGE 28 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE of Responsible Care®. This would reduce the regulatory power the chemical industry now exclusively holds, make it more accountable for and attentive to potential sources of environmental and occupational ill health. Furthermore, the 2001 impasse with respect to a global agreement on Responsible Care® (discussed in response to Question Three) should be overcome. Here, the global Responsible Care® leadership should apply pressure on the ACC to compromise with the international union association ICEM and agree upon a draft international resolution. The new sense of urgency around toxic exposure and chemical security post 9/11 should be leveraged as an impetus to bring all stakeholders back to the table. Responsible research, interventions and policy outside Responsible Care® Alternative industrial codes have been unpopular in the US (71)even though there is a significant degree of overlap between them and Responsible Care® (13,42). While selfregulation may be the tipping point in companies endorsement of industrial codes, more comparative research is needed to determine which codes produce the best health outcomes internationally and how they can be made more popular and relevant in the US context. This, again, is an attempt to bridge the divide between reputational and physical commons discussed earlier. Moreover, additional research involving multiple stakeholders in the chemical industry (such as vendors, policymakers, community members, and environmental experts) could reveal pathways to bridging this divide. Research could focus not only on stakeholder perspectives on industrial codes, but their ideas on how to realistically improve them. Once published, this research may be used to leverage public opinion and motivate the chemical industry to improve its practices. The involvement of worker unions in the Responsible Care® process has taken place in other countries (mostly European) (49) but not in the US. While there is a strong degree of PAGE 29 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE QUESTION FIVE antagonism between the chemical industry and the union movement, unions have been able to leverage regulations around occupational health and safety, particularly at the state level (72,73). US unions could perhaps devise or adapt an industrial workers code based on their interests based on the premise of occupational health and consultations with their international counterparts to lobby the government for support. Thus, a code created as an intervention could become institutionalized as policy on the state level, and eventually affect industry on the federal level. While this involves expending large amounts of resources, in the long term, it may prove cost effective for unions, especially considering the number of occupational accidents that continue to occur in the chemical industry (15,51). Bridging the “Physical-Reputational” Commons: Purposeful Research as the best next step Public opinion has been a driving force behind reform in the chemical industry; research can play an important role in shaping public opinion. As mentioned earlier, a significant gap in international research is around the Responsible Care® programs of US-based industries in the developing world. The next best step is to take advantage of these three facts. Schools of Public Health and Business in credible institutions such as Johns Hopkins and MIT should divert their research dollars towards looking at incidences of exposure, health outcomes, and management practices associated with Responsible Care® multinational facilities all over the world. The emphasis should be on developing strong research methodologies to make well-substantiated conclusions about an environmental health “story” that the media can pitch to the public. Thus, research can feed the media, driving drive public opinion which could apply pressure on the ACC to improve the practices of Responsible Care® across the board. In this way, researchers are uniquely positioned to initiate the bridging of physical and reputational commons to improve industrial standards and codes across the world and reduce the global risk of toxic environmental exposure. Indeed, the legacy of Bhopal demands it. PAGE 30 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE LITERATURE CITED (1) Broughton E. The Bhopal disaster and its aftermath: a review. Environmental Health 2005 May 10; 4(1): 6. (2) Dhara VR, Dhara R. The Union Carbide disaster in Bhopal: a review of health effects. Archives of Environmental Health 2002 Sep-Oct; 57(5): 391-404. (3) Mehta PS, Mehta AS, Mehta SJ, Makhijani AB. Bhopal tragedy's health effects. A review of methyl isocyanate toxicity. JAMA: the journal of the American Medical Association 1990 Dec 5; 264(21): 2781-2787. (4) Fact Finding Mission on Bhopal (SRISHTI). 2002. (5) Ranjan N, Sarangi S, Padmanabhan VT, Holleran S, Ramakrishnan R, Varma DR. Methyl isocyanate exposure and growth patterns of adolescents in Bhopal. JAMA: the journal of the American Medical Association 2003 Oct 8; 290(14): 1856-1857. (6) Cullinan P, Acquilla S, Dhara VR. Respiratory morbidity 10 years after the Union Carbide gas leak at Bhopal: a cross sectional survey. The International Medical Commission on Bhopal. BMJ (Clinical research ed.) 1997 Feb 1; 314(7077): 338-342. (7) Dhara VR. What ails the Bhopal disaster investigations? (And is there a cure?). International Journal Of Occupational And Environmental Health: official journal of the International Commission on Occupational Health 2002 Oct-Dec;8(4): 371-379. (8) World Health Organization. Gender and Health in Disasters. 2002. (9) BBCi. Risk in Industrial Society - Some Case Histories. 2002; Available at: http://www.bbc.co.uk/dna/h2g2/A784109. Accessed 13th June, 2005. (10) US Congress. Emergency Planning & Community Right to Know Act. 1986;42 U.S.C. 11001 et seq. (11) Munn K. Responsible Care and Related Voluntary Initiatives to Improve Enterprise Performance Of Health, Safety And Environment in The Chemical Industry. 2000. International Labor Organization Sectoral Program. (12) International Labor Organization. ILO SafeWork - Chemical Safety - 20 years after Bhopal. 2004; Available at: http://www.ilo.org/public/english/protection/safework/chemsfty/bhopal/. Accessed June 13, 2005. (13) Nash J, Ehrenfeld J. Codes of Environmental Management Practice: Assessing their Potential as a Tool for Change. Annu Rev Energy Environ 1997;22:487-535. (14) Kaye WE, Orr MF, Wattigney WA. Surveillance of hazardous substance emergency events: identifying areas for public health prevention. International journal of hygiene and environmental health 2005;208(1-2):37-44. PAGE 31 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE LITERATURE CITED (15) National Response Center. NRC Statistics - Incident Types. 2005; Available at: http://www.nrc.uscg.mil/incident97-02.html. Accessed June 13, 2005. (16) Schulz A, Northridge ME. Social determinants of health: implications for environmental health promotion. Health education & behavior : the official publication of the Society for Public Health Education 2004 Aug;31(4):455-471. (17) Alleyne G. Foreward . In: Merson MH, Black RE, Mills AJ, editors. International Public Health: Diseases, Programs, Systems, and Policies. 2nd ed. Sudbury, MA: Jones & Bartlett Publishers; 2005. p. xiii-v. (18) Poland B, Coburn D, Robertson A, Eakin J. Wealth, equity and health care: a critique of a "population health" perspective on the determinants of health. Critical Social Science Group. Soc Sci Med 1998 Apr;46(7):785-98. (19) Navarro V, Shi L. The political context of social inequalities and health. Soc Sci Med 2001 Feb;52(3):481-91. (20) Starfield B. Improving equity in health: a research agenda. International journal of health services : planning, administration, evaluation 2001;31(3):545-566. (21) Krieger N, Williams DR, Moss NE. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health 1997;18:341-78. (22) Wilkinson RG. Unhealthy societies : the afflictions of inequality. London ; New York: Routledge; 1996. (23) Beaglehole R, Bonita R. Reinvigorating public health. Lancet 2000 Sep 2;356(9232):787788. (24) Navarro V. Health and equity in the world in the era of "globalization". International Journal of Health Services : planning, administration, evaluation 1999;29(2):215-226. (25) Schuftan C. Equity in health and economic globalisation. Dev.Pract. 1999 Nov;9(5):610614. (26) Yach D. 'Health-for-All' in the twenty-first century: a global perspective. The National Medical Journal of India 1997 Mar-Apr;10(2):82-89. (27) Setlow V, Lawson CE, Woods NF, Institute of Medicine . Committee on Gender Differences in Susceptibility to Environmental Factors. Gender differences in susceptibility to environmental factors : a priority assessment : workshop report. Washington, D.C.: National Academy Press; 1998. (28) Sims J, Butter ME. Gender Equity and Environmental Health. 2000. Gender and Health Equity Series. Harvard Center for Population and Development: Cambridge, MA. PAGE 32 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE LITERATURE CITED (29) Ohayo-Mitoko GJ, Kromhout H, Karumba PN, Boleij JS. Identification of determinants of pesticide exposure among Kenyan agricultural workers using empirical modeling. The Annals of Occupational Hygiene 1999 Nov; 43(8): 519-525. (30) Denham M, Schell LM, Deane G, Gallo MV, Ravenscroft J, DeCaprio AP, et al. Relationship of lead, mercury, mirex, dichlorodiphenyldichloroethylene, hexachlorobenzene, and polychlorinated biphenyls to timing of menarche among Akwesasne Mohawk girls. Pediatrics 2005 Feb; 115(2): 127-34. (31) Weisskopf MG, Wright RO, Schwartz J, Spiro A,3rd, Sparrow D, Aro A, et al. Cumulative lead exposure and prospective change in cognition among elderly men: the VA Normative Aging Study. American Journal of Epidemiology 2004 Dec 15; 160(12):1184-1193. (32) Children's Environmental Health Network. An Introduction to Children's Environmental Health. n.d.; Available at: http://www.cehn.org/cehn/WhatisPEH.html. Accessed June 13th, 2005. (33) Malcoe LH, Lynch RA, Keger MC, Skaggs VJ. Lead sources, behaviors, and socioeconomic factors in relation to blood lead of native American and white children: a community-based assessment of a former mining area. Environmental health perspectives 2002 Apr;110 Suppl 2:221-231. (34) Krieger J, Higgins DL. Housing and health: time again for public health action. American Journal of Public Health 2002 May; 92(5): 758-768. (35) Brown MJ, Gardner J, Sargent JD, Swartz K, Hu H, Timperi R. The effectiveness of housing policies in reducing children's lead exposure. American Journal of Public Health 2001 Apr; 91(4): 621-624. (36) Butler M. Lessons from Thor Chemicals. In: Bethlehem L, Goldblatt M, editors. The Bottom Line: Industry and the Environment in South Africa Ottawa, Canada: International Development Research Centre/UCT Press; 1997. (37) Davanzo F, Settimi L, Faraoni L, Maiozzi P, Travaglia A, Marcello I. Agricultural pesticide-related poisonings in Italy: cases reported to the Poison Control Centre of Milan in 2000-2001. Epidemiologia e prevenzione 2004 Nov-Dec; 28(6): 330-337. (38) Stern AH. A review of the studies of the cardiovascular health effects of methyl mercury with consideration of their suitability for risk assessment. Environmental research 2005 May; 98(1):133-142. (39) Ushijima K, Kitano T, Shono M, Oka T, Miyake Y, Moriyama M, et al. Social factors associated with psychological distress among inhabitants in a methyl-mercury polluted area in rural Japan. Environ.Sci. 2004; 11(3):151-162. (40) US Department of Labor Occupational Safety & Health Administration. OSHA 30-Year Milestones. n.d.; Available at: http://www.osha.gov/as/opa/osha30yearmilestones.html. Accessed June 13, 2005. PAGE 33 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE LITERATURE CITED (41) Brown G. Global Threats to Workers' Health and Safety on the Job. Social Justice 2002;29(3):n/a. (42) Nash J, Ehrenfeld JR. Factors that shape EMS outcomes in firms. In: Coglianese C, Nash J, editors. Regulating from the Inside: Can Environmental Management Systems Achieve Policy Goals? Washington, DC: Resources for the Future; 2001. p. 61-81. (43) Meister D. Lax workplace-injury policies are killing us. San Francisco Examiner 2002 April 25 2002. (44) International Council of Chemical Associations. Responsible Care: Who We Are. n.d.; Available at: www.responsiblecare.org. Accessed June 13, 2005. (45) Synthetic Organic Chemical Manufacturers Association (SOCMA). Synthetic Organic Chemical Manufacturers Association (SOCMA) - Responsible Care - Guiding Principles. ; n.d. (46) American Chemistry Council. American Chemistry Council - Public Website. n.d.; Available at: http://www.americanchemistry.com/cmawebsite.nsf. Accessed June 13, 2005. (47) American Chemical Company. Responsible Care Security Code of Management Practice. ; n.d. (48) Chemical Industry Archives. Responsible? Care?: As bad news mounts and polls head south, chemical companies spend millions on 'public perception'. 2001; Available at: http://www.chemicalindustryarchives.org/dirtysecrets/responsiblecare/1.asp. Accessed June 13, 2005. (49) International Council of Chemical Associations (ICCA). Industry as a partner for sustainable development - Chemicals. 2002; Report prepared for the United Nations Environment Program. Geneva, Switzerland: ICCA. (50) Prakash A. Responsible Care: An Assessment. Business & Society 2000 June;39(23):183209. (51) Purvis M, Bauler J. IRRESPONSIBLE CARE The Failure of the Chemical Industry to Protect the Public from Chemical Accidents. 2004 April:1-2281. (52) King A, Lenox M. Industry self-regulation without sanctions: the chemical industry's Responsible Care Program. Academy of Management Journal 2000;43(4):698-716. (53) Synthetic Organic Chemical Manufacturers Association (SOCMA). Synthetic Organic Chemical Manufacturers Association (SOCMA) - Responsible Care - Products. ; n.d. (54) Walt G. Global Cooperation in International Public Health. In: Merson M, Black RE, Mills AJ, editors. International Public Health: Diseases, Programs, Systems, and Policies. 2nd ed. Sudbury, MA: Jones & Bartlett Publishers; 2005. p. 667-699. PAGE 34 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE LITERATURE CITED (55) Ιnternational Federation of Chemical, Energy, Mine and General Workers' Unions (ICEM). Responsible Care: Unions' New Offer to Chemical Employers. ICEM Update 2001(91/2001):June 14, 2005. (56) Bossong-Martines E. Chemicals: Basic. Standard & Poor's Industry Surveys 1999;167(2). (57) Olson M. The Logic of Collective Action: Public Goods and the Theory of Groups. Cambridge, MA: Harvard University Press; 1965. (58) Gupta A, Lad L. Industry self-regulation: An economic, organizational, and political analysis. Academy of Management Review 1983;8:416-25. (59) Cohen N, Chess C. Fostering Environmental Progress: A Case Study of Vulcan Chemical's Community Involvement Group. New Brunswick, NJ: Center for the Environment and Communities, Cook College, Rutgers University; 1995. (60) Cohen N, Chess C. Improving Dialogue: A Case Study of the Community Advisory Panel of Shell Oil Company's Martinez Manufacturing Complex. New Brunswick, NJ: The Center for Environment and Management, Cook College, Rutgers University; 1995. (61) Lynn F, Chess C. Community advisory panels with the chemical industry: antecedents and issues. Bus Strategy Environ 1994; 3(2): 92-9. (62) Howard A. The Environmental Transformation of American Industry: An Institutional Account of Organizational Evolution in the Chemical and Petroleum Industries (1960-1993). 1995. (63) Nash J. Industry Codes of Practice: Emergence and Evolution. In: Dietz T, Stern P, editors. New Tools for Environmental Protection: Education, Information, and Voluntary Measures Washington, DC: National Academy Press; 2002. (64) Rogers EM. Diffusion of innovations. 4th ed. New York: Free Press; 1995. (65) US Environmental Protection Agency Science Advisory Board. Commentary Resulting from a Workshop on the Diffusion and Adoption of Innovations in Environmental Protection. 2000 November;EPA-SAB-EEC-COM-01-001:A1-A15. (66) Hoffman A. Institutional evolution and change: Environmentalism and the US chemical industry. Academy of Management Journal 1999; 20: 1015-52. (67) LaPlante A. Trust Us, Don't Track Us: An Investigation of the Chemical Industry's Responsible Care Program. 1998. (68) Lenox M, Nash J. Industry Self-Regulation and Adverse Selection: A Comparison Across Four Trade Association Programs. Bus Strategy Environ 2003;12:343-56. (69) DowAgro. Responsible Care. n.d; Available at: http://www.dowagro.com/india/responsible/ Accessed June 16, 2005 PAGE 35 OF 36 STUDENT ID #: 413 PROBLEM AREA THREE – TOXIC ENVIRONMENTAL EXPOSURE LITERATURE CITED (70) Bayer Corporation. Bayer AG - Sustainable Development Report 2004 - Homepage. 2004; Available at http://www.sd.bayer.com. Accessed June 16, 2005 (71) Prakash A. A new-institutionalist perspective on ISO 14000 and Responsible Care. Bus Strategy Environ 1999;8:322-5. (72) International Union of Operating Engineers Local 30. NYS AFL-CIO: Labor can be proud of 2003 legislative accomplishments . n.d.; Available at: http://www.iuoe30.org/news/2003_accomplishments.htm. Accessed June 17, 2005. (73) Massachusetts AFL-CIO. Legislative Department: working for the best interests of working families. n.d.; Available at: http://www.massaflcio.org/legislativedepartment.asp. Accessed June 17, 2005. (74) Link BG, Phelan J. Social conditions as fundamental causes of disease. J Health Soc Behav 1995;Spec No:80-94. (75) Union Carbide Corporation. History. n.d.; Available at: http://www.unioncarbide.com/history/. Accessed June 14, 2005. PAGE 36 OF 36