Case 3 - Pathology
advertisement

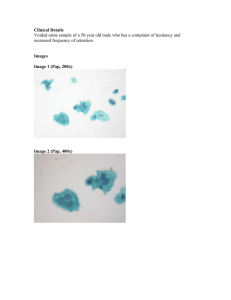
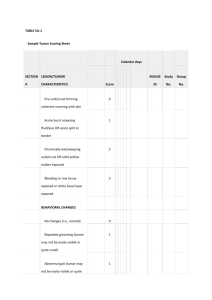
SP web 52007 A 77 year female was noted to have a bladder lesion on the posterior wall. Choose the correct diagnosis: A. B. C. D. Signet ring cell carcinoma Clear cell (mesonephric) adenocarcinoma Nephrogenic adenoma Metastatic thyroid carcinoma Answer: C Histological description: There are two pieces of tissue removed. One piece consists of tubules lined by cuboidal flattened epithelium with dense pink secretions resembling thyroid follicles. Many of the follicles have associated intraluminal acute inflammation. The other piece of tissue shows a mixture of small tubules and structures resembling signet ring cells containing blue tinged mucinous secretions. Some of the small tubules and signet ring-like structures have a hyaline rim of collagen surrounding them. Both pieces of tissue on the surface are lined by flat cuboidal epithelium. Discussion: This is a classic case of nephrogenic adenoma. Nephrogenic adenoma may have multiple histological patterns. Some of them, like the signet ring-like cell pattern, may be confused with adenocarcinoma, yet other patterns will typically be present, providing a clue to the correct diagnosis. In this case the thyroid-like tubules are particularly striking and is a characteristic feature of nephrogenic adenoma not seen with any of its mimickers. The signet-ring-like structures represent small tubules lined by flattened epithelium which depending on the plane of section may show only one nucleus resembling a signet ring cell carcinoma. Distinguishing it from signet ring cell carcinoma requires finding of slightly larger similar tubules with more than one nucleus, the hyaline rim of connective tissue surrounding some of these structures, and the other more characteristic features of nephrogenic adenoma seen elsewhere in the lesion. Features that should not be seen in nephrogenic adenoma include mitotic figures or necrosis. While I have seen rare cases with very focal clear cells and small solid nest of cells these are distinctly uncommon and more typically seen in malignant tumors resembling nephrogenic adenoma such as clear cell (mesonephric) adenocarcinoma. Case 2 A 71 year old male underwent a transurethral resection of the prostate for lower urinary tract symptoms. Choose the correct diagnosis: A. Basal cell hyperplasia. B. Basal cell carcinoma. C. Adenocarcinoma of the prostate. Answer A. Histological description This entire TURP consisting of 12 slides was entirely involved by the process illustrated. There are numerous crowded medium sized glands some arranged in a lobular configuration and others appearing more diffusely infiltrative. The glands show an inner layer of cells with abundant lightly eosinophilic cytoplasm associated with benign appearing nuclei. Many of the glands contain dense pink secretions. Exterior to the inner secretory cell lining is a proliferation of cells with enlarged nuclei containing very prominent nucleoli with scant cytoplasm. These cells range from one cell thick to several cells in thickness. These nuclei are blue-gray in contrast to the more violet appearing nuclei of the overlying secretory cells. Focally within this process there are occasional cribriform glands with a similar inner lining of benign secretory cells and an exterior proliferation of cells with enlarged nuclei containing prominent nucleoli. Within the cribriform lumina there are basophilic secretions. Discussion: This pattern of basal cell hyperplasia is particularly difficult to distinguish from adenocarcinoma of the prostate. The more easily recognizable form of basal cell hyperplasia consists of tubules with a more prominent piling up of basal cell layer including solid nests of basal cells, distinctive from adenocarcinoma of the prostate. In contrast, this case shows only minimal piling up of the basal cell layer along with a crowded glandular proliferation more closely mimicking prostate cancer. The key distinguishing feature is the two distinct cell layers with both a basal layer and an overlying secretory cell layer. Basal cells may show prominent nucleoli in both normal basal cells as well as in basal cell hyperplasia, as seen in the current case. This case also shows focal cribriform basal cell hyperplasia which could mimic one of the patterns of basal cell carcinoma. However the presence of the overlying secretory cell layer both in the cribriform glands as well as in the tubular glands is not a feature of basal cell carcinoma. Furthermore, basal cell carcinoma tends to show a desmoplastic stromal reaction which is lacking in the current case. Despite the extensive nature of this process, this lesion is entirely benign and merely a mimicker of prostate cancer. Case 3 An 81 year old female was noted to have a bladder lesion. Choose the correct diagnosis: A. B. C. D. Papillary urothelial hyperplasia. Urothelial dysplasia with early papillary formation. Urothelial papilloma. Low grade papillary urothelial carcinoma. Answer B. Histological description This lesion consists of urothelium which is normal in thickness thrown into papillary folds. A few underlying nests are present representing their involvement of Von Brunn nests or a tangential sectioning. Scattered nuclei are enlarged showing some variability in size and shape. An accompanying ck20 stain showed full thickness positivity. Discussion This lesion has the overall growth pattern of papillary urothelial hyperplasia. The distinction between papillary urothelial hyperplasia and a papillary neoplasm such as papilloma or low grade papillary carcinoma is that in the latter there are well formed distinct papillary fronds. In a papillary urothelial neoplasm the papillary formations are complex with branching such that sectioning of the lesion results in the histological appearance of fronds that appear to be dissociated from the underlying mucosa. In contrast with papillary urothelial hyperplasia there are simple folds within the mucosa such that sectioning does not give rise to a frond composed of a fibrovascular core circumferentially surrounded by urothelium appearing to be “floating” separate from the underlying mucosa. In a typical case of papillary urothelial hyperplasia there is a lack of cytologic atypia. However in the current case there is pleomorphism warranting a diagnosis of dysplasia yet not up to the level of carcinoma in-situ. The presence of full thickness ck20 positivity supports the presence of dysplasia as opposed to reactive or normal urothelium. Papillary urothelial hyperplasia in many cases represents a precursor lesion to papillary urothelial neoplasms. The presence of dysplasia with early papillary formation is even more worrisome for the heralding of subsequent papillary urothelial neoplasms. If this is the first manifestation of urothelial disease in this patient, close clinical follow up would be warranted. Case 4 A 49 year old male was noted to a paratesticular mass. A frozen section was performed. Choose the correct diagnosis A. Adenomatoid tumor. B. Metastatic adenocarcinoma. C. Sertoli cell tumor. D. Epithelioid hemangioendothelioma. Answer A. Histological description Adjacent to the testis is a mass consisting of nests and cords of cells with abundant eosinophilic cytoplasm. Many of the cells contain a clear cytoplasmic vacuole. The nuclei are enlarged with prominent nucleoli. The background appears to be fibrotic. Focally the lesion extends into the testis invading in between seminiferous tubules. Elsewhere the lesion shows central infarction. Discussion One of the keys to recognizing this entity is its paratesticular as opposed to intratesticular location. Relatively few entities involved the paratesticular region, with adenomatoid tumor being one of the most common. Although these lesions may focally invade the testis as seen in the current case, it is extremely rare for them to be totally intratesticular. These lesions resemble epithelioid hemangioendothelioma in that they consist of cords or nests of cells with vacuole formation. However no red blood cells are noted within the vacuoles. An unusual but well recognized feature seen in the current case is the central infarction. (Am J Surg Pathol 28; 77-83, 2004). Recognition of this lesion at the time of frozen section may spare a patient orchiectomy as localized excision is adequate. Diagnosis on permanent sections is more readily accomplished as one can perform immunostains for calretnin demonstrating the lesion’s mesothelial origin. Although this lesion is a mesothelioma, because adenomatoid tumor is a well described clinicopathological entity and because the diagnosis of mesothelioma in this region has the connotation of malignancy, these lesions are still noted as adenomatoid tumors rather than mesotheliomas. Case 5 A 20 year old male was noted to have a testicular mass and underwent orchiectomy. Choose the correct diagnosis A. Choriocarcinoma and teratoma. B. Teratoma with prominent syncytiotrophoblastic giant cells. C. Embryonal carcinoma. Answer A. Histological description Some of the tumor is characterized by tubules lined by cuboidal epithelium as well as epithelium with columnar cells showing subnuclear vacuoles. Elsewhere there are areas of necrosis and hemorrhage surrounded by very pleomorphic cells. In areas a dimorphic population may be recognized consisting of multinucleated cells with abundant amphophilic cytoplasm and very pleomorphic nuclei adjacent to cells with smaller yet still recognizably malignant nuclei with slightly grayer cytoplasm. Discussion This case is a nice example of choriocarcinoma in a malignant mixed germ cell tumor. It is relatively rare to see choriocarcinoma as a component of a mixed germ cell tumor. More frequently, one can see scattered syncytiotrophoblastic giant cells in a setting of seminoma or less frequently embryonal carcinoma or teratoma. The distinction between isolated syncytiotrophoblastic giant cells and choriocarcinoma is the presence of cytotrophoblasts in choriocarcinoma. In cases with only isolated syncytiotrophoblastic giant cells the giant cells tend to cluster around blood lakes and dilated blood vessels further mimicking choriocarcinoma. However in choriocarcinoma one tends to see not only tumor surrounding areas of hemorrhage but areas of frank necrosis as well. Although pathologists tend to worry about missing small foci of choriocarcinoma in a malignant mixed germ cell tumor, this is not a critical issue in terms of treatment or prognosis. In a non seminomatous germ cell tumor, the prognosis is based more on serum markers than on the histological findings. This includes levels of alpha fetoprotein, HCG, and LDH. In addition whether there are non-pulmonary visceral metastases is also of prognostic significance. As it relates to trophoblastic cells, the presence of a HCG level less than 5000 IU/L is of good prognosis as compared to an intermediate prognosis with HCG levels between 5000 and 50,000 and a poor prognosis with HCG levels greater than 50,000. Consequently, cases with scattered syncytiotrophoblastic giant cells or even small foci of choriocarcinoma will typically have HCG levels of less than 5000 with a good prognosis regardless whether there is choriocarcinoma present or absent. In cases with a more significant choriocarcinoma component, there will be more markedly elevated HCG levels in the serum with a correspondingly worse prognosis. Case 6 A 55 year old male was noted to have a paratesticular lesion. Choose the correct diagnosis A. B. C. D. Leiyomyoma. Adenomatoid tumor with smooth muscle hyperplasia. Low grade leiyomyosarcoma. High grade leiyomyosarcoma. Answer C. Histological description The lesion consists of fasicles of spindle cells with abundant eosinophilic cytoplasm. The nuclei are elongated and cigar shaped. Many of the nuclei appear relatively uniform without significant pleomorphism. Other areas show more striking nuclear pleomorphism. Mitotic figures are rare with no evidence of necrosis. The lesion is of moderate cellularity. Discussion In an adult, the most common paratesticular soft tissue tumor is liposarcoma, typically well differentiated. Paratesticular leiomyosarcomas are less frequently present. Although adenomatoid tumors of the testis may show a very prominent smooth muscle component one still will be able to identify the epithelial component of an adenomatoid tumor which is lacking in the current case. Also the presence of atypia in the current case rules out leiomyoma and smooth muscle hyperplasia with an adenomatoid tumor. Although there is striking cytologic atypia, the overall cellularity is not high, mitotic figures are not frequent, and the lesion lacks necrosis such that it would be best regarded as low grade leiomyosarcoma. In a study from our institution, the key prognostic feature is the grade of the tumor. All patients with low grade leiomyosarcomas were alive without evidence of disease although a couple of patients experienced local recurrences. In contrast all of the high grade leiomyosarcomas were dead of disease. Therapy typically consists of radical orchiectomy. Immunohistochemically these lesions express muscle markers as in other sites. The only pitfall that one must be aware of is as with leiomyosarcomas elsewhere, some of these lesions may show focal expression for cytokeratin.