Natural History of Uncomplicated Cellulitis
advertisement

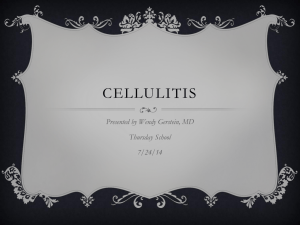
CELLULITIS Introduction ● Cellulitis is an extremely common presentation to the Emergency Department. The term “cellulitis” is commonly used to indicate an uncomplicated nonnecrotizing inflammation of the dermis and hypodermis related to acute infection that does not involve the fascia or muscles, and that is characterized by localized pain, swelling, tenderness, erythema, and warmth. 2 ● It is important to understand the natural history of uncomplicated cellulitis when planning management. ● The most serious differential diagnosis will be a rapidly progressive necrotising infection, (necrotizing fasciitis or clostridial myonecrosis) ● The most common differential diagnosis will be lipodermatosclerosis. Pathophysiology Organisms: Cellulitis is usually caused by: ● Streptococcus pyogenes. ● Staphylococcus aureus. Natural History of Uncomplicated Cellulitis: ● The natural history of cellulitis is for progression of erythema and a persistent temperature up to 72 hours after the commencement of appropriate antibiotic therapy. ● The erythema will then gradually resolve over a period of weeks, however some patients will have persistent discoloration for many months. Clinical Features The patient will usually seek medical assistance within 48 hours of the onset of symptoms. Cellulitis usually presents with the acute onset of: ● Fever. ● Painful erythematous area of skin inflammation. ● Tenderness over the involved site. ● The most common site of involvement will be the lower leg. Differential Diagnoses: Differential diagnoses include: 1. Lipodermatosclerosis ● This is a common condition that results in chronic erythema and pain in the lower limbs. It is associated with chronic venous insufficiency and is often bilateral. Episodic exacerbations of pain and erythema are commonly confused with cellulitis. Bilateral involvement and the absence of systemic symptoms are useful pointers to differentiate this condition from cellulitis. Left, typical appearance of streptococcal cellulitis. Right, typical appearance of lipodermatosclerosis 2. Erythema Nodosum 3. Drug reaction 4. Burns ● 5. This will be self evident on history, however in some confused patients the diagnosis may be more problematic. Rapidly progressive necrotizing infection ● Otherwise known by the terms, necrotizing fasciitis and gas gangrene, this is the most important differential diagnosis as it is a life threatening condition. ● It is suggested by involvement of subcutaneous tissues with subcutaneous induration, obvious necrosis or gas, severe pain, bullous skin changes, haemorrhage rapid progression, severe sepsis, ongoing rigors, perineal or abdominal location. ● The external signs may initially be deceptively minimal, however the patient will usually be systemically unwell. See separate guidelines for necrotizing fasciitis and gas gangrene. Management Patients are commonly referred to hospital by their GPs for intravenous antibiotic therapy after “failure of oral antibiotic therapy” as they have had spreading erythema or ongoing fever soon after starting oral antibiotics. It is important to realize that the presence of these features in a patient who is otherwise clinically improving does not necessarily indicate a failure of oral therapy. This includes patients who are febrile, may have had an isolated episode of rigor or have evidence of lymphangitis. Oral antibiotic therapy is suitable for most adult patients with uncomplicated cellulitis. Antibiotics Oral antibiotics: NOTE: antibiotic doses below refer to adults with normal renal and hepatic function. Consider alternative antibiotics for patients with water related infections (see also latest Antibiotic Therapeutic Guidelines). Oral antibiotic therapy with LMO follow up. ● Oral flucloxacillin 1g qid or cephalexin 1g qid may be used ● In patients with immediate penicillin hypersensitivity use clindamycin 450mg orally tds. IV Antibiotics for Admitted patients: ● Patients admitted to the ward may be commenced on cefazolin 1 to 2g IV tds or flucloxacillin 1to 2g IV qid. ● In patients with immediate penicillin hypersensitivity use clindamycin 450mg IV tds or vancomycin 1g IV bd. Disposition considerations Patients who require hospital admission: The following situations will require hospital admission: 1. Patients with significant co-morbidities: ● In particular patients who are immunosuppressed. 2. Patients unable to tolerate oral medication. 3. Patients who are not able to organize or are not suitable for GP review: ● 4. Complicated cellulitis: ● 5. 7. 8. Patients who are systemically unwell, (hypotension or other signs of severe sepsis). Cellulitis complicating trauma: ● 6. In particular patients with social issues that would be expected to significantly impact on care. Especially if associated with penetrating injuries, (may need surgical debridement). More serious underlying infection is suspected, such as: ● Necrotising fasciitis or clostridial myonecrosis in particular, (see above) ● Underlying abscess formation. Special sites: ● Periorbital cellulitis ● Perineal cellulitis Children: ● If there are any concerns, these patients should be discussed with the pediatric unit. Admitting Unit Considerations: Medical Unit: ● Most patients who do require hospital admission should be admitted under a medical unit. SSU: ● Some patients may be suitable for an SSU admission. HITH: ● Patients who are well enough to be treated at home are usually well enough to receive oral antibiotic therapy. ● An example of a patient that may require management by a “Hospital in the Home Unit” is one who has limited cellulitis and mild to moderate systemic symptoms but for some reason cannot take oral antibiotics. Surgical Unit: A surgical consultation must be sought for any patient who may potentially require surgery, including: ● Patients suspected of having a rapidly progressing necrotizing infection. ● Patients with cellulitis involving the face or the hands, (these will generally be seen by the Plastics unit) ● Cellulits associated with penetrating trauma, (unless of a minor nature). Ophthalmology: ● Cases of periorbital cellulitis should be referred to the ophthalmology unit. References: 1. Antibiotic Therapeutic Guidelines 13th ed 2006 2. May AK. Skin and soft tissue infections. Surg Clin North Am. Apr 2009; 89(2): 403-20 Dr J. Hayes. Dr Craig Aboltins/ Dr Peter Stanley Infectious Disease Physicians, Northern Hospital Dr Rabin Sinnappu, HITH Physician Reviewed June 2010