Musculoskeletal 1a – Muscle Disease
advertisement

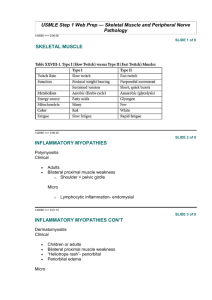
Musculoskeletal 1a – Muscle Disease Anil Chopra 1 Primary muscle diseases comprise: - muscular dystrophies - Congenital myopathies 2 Pathogenesis of muscle weakness - progressive muscle degeneration and fibroadipose tissue substitution in muscular dystrophy: - Reduced force generated by muscle in congenital myopathies but little or no change with time 3 Main group of proteins involved in muscular dystrophies - the dystrophin-associated glycoprotein complex - (laminin/ dystroglycan/ sarcoglycans/ dystrophin) 4 Main group of proteins involved in congenital myopathies - Proteins of sarcomeres (actin, tropomyosin and nebulin) 5 Main clinical features of the muscular dystrophies: - proximal weakness - joint contractures respiratory muscle involvement Neuromuscular Disorders Many are inherited Various parts of the motor units affected A defect in a motor neuron or nerve is a neuropathy A defect at the neuromuscular junction is a myasthenia. A defect of muscle is a myopathy. Myopathies 1. Congenital myopathies 2. muscular dystrophies Congenital Myopathies General Features - non progressive - weakness from birth or infancy - generally, patients achieve the ability to walk independently - serum creatine kinase are normal only mildly elevated, indicating low degree of muscle damage. - Characterised by generalised muscle thinning and muscle weakness. - Respiratory muscle weakness can be out of proportion compared to limb muscle weakness. There are 4 types of congenital myopathies - central core disease o disturbance of excitation contraction coupling - nemaline myopathy o sarcomeric protein diseases - myotubular myopathy o problems in cell-cell signalling and energy metabolism - minicore myopathy o disturbance of excitation contraction coupling Severity depends on the degree of disruption of the excitation/contraction coupling or the degree of defect in the sarcomeric proteins. Generally symptoms are mild: Proximal muscle weakness: o difficulties in walking fast o difficulties in running o difficulties in getting up from the floor Axial weakness: o scoliosis common o respiratory muscle weakness common even in ambulant patients Proteins Affected Nebulin Alpha-actin Beta tropomyosin (TPM2) Alpha tropomyosin 3 (TMP3) Troponin T1 (TNNT1) Muscular Dystrophies Histological Assessment - Wide variations in fibre size - Necrosis - Fibrosis, fat - Hypercontracted fibres - Split fibres whorled fibres - internal nuclei - basophilic fibres Muscular dystrophies can be congenital or onset during childhood, and rarely in adulthood. They are characterised by: - Often progressive weakness - Variable severity: from congenital to adult onset depending on the subtype (many subtypes recognised) - Weakness o usually proximal o rarely distal - Respiratory muscle weakness - Limitation of joint movements often accompanies the weakness - Muscle atrophy often with associated pseudohypertrophy in the same patient. There are different muscle proteins involved with muscular dystrophies than with myopathies. The ones affected in muscular dystrophy include: 1. Transarcolemma (Duchenne, sarcoglycanopathies, others) 2. Enzymes 3. Nuclear envelope 4. Extracellular matrix 5. Sarcomere 6. Others (cytoskeleton; ER proteins of unknown) Deficiencies in extracellular proteins cause congenital muscular dystrophies. E.g. merosin deficiency, collagen VI deficiency causes “Ulrich congenital muscular dystrophy”. They are characterised by random contractures at birth – arthrogryposis. Sarcoglycanopathies: deficiencies in sarcoglycans. Duchenne Muscular Dystrophy Caused by a deficiency in the dystrophin molecule. 1 in 3500 male births symptomatic <1 year - 5 years loss of independent walking 6 -12 years death mid teens - early twenties 30% significant learning difficulties Molecular Basis Duchenne is caused by abnomailities in chromosome 21 which codes for the dystrophin protein. An “in frame” deletion causes fewer complications than an “out of frame” deletion. NH CY S 2 COOH Full length protein NH Truncated and unstable protein 2 out of frame deletion Clinical Presentation: late walking - 50% >18 months toe walking unable to run or jump falls CY S CO OH stairs and climbing hard Gowers’ Manoeuvre – getting up by rolling onto their front and using their arms. IQ shifted -1SD 30% IQ<70, mean IQ 85 verbal IQ < performance IQ speech delay very common Later Presentatons Progressive joint contractures Progressive scoliosis Dilated cardiomyopathy Weakness of the inspiratory and expiratory muscles: this is particularly dangerous as it can lead to o frequent respiratory infections o nocturnal hypoventilation o nocturnal hypoxia o nocturnal hypercarbia (too much CO2) o morning drowsiness, headaches, nausea, fatigue o respiratory insufficiency and sudden death Diagnosis – the diagnosis of Duchenne’s is difficult and is often untreatable. • CK: 50 - 100x normal • deletion in gene detectable in 70% • muscle biopsy – histology dystrophic – immunocytochemistry shows absent dystrophin Treatment - using ACE inhibitors can slow the onset of dilated cardiomyopathy - β- blockers are becoming increasingly used Becker Muscular Dystrophy Presentation • Mean age of onset of symptoms is around 11 yrs • Calf pains, slower than peers • Variable progression • Loss of walking ability – only in 18% (Mean age at loss of walking – 37 yrs) • Scoliosis extremely uncommon • Dilated cardiomyopathy however very common. Molecular Basis Generally only caused by “in frame” deletions leaving a partially functional protein. NH CYS COOH Full length protein CY S COO H Shorter but partially functional protein 2 N H 2 in frame deletion