Pediatric Rehabilitation and Duchenne Muscular
advertisement

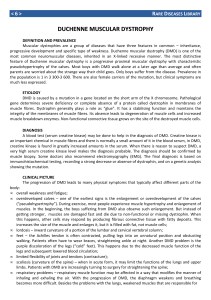
Kara Altland November 15, 2013 PT 100 Dr. Glumac Computer Library Project Pediatric Physical Therapy and Duchenne Muscular Dystrophy Duchenne muscular dystrophy (DMD) is a recessive disorder, most commonly seen in boys. It has been linked to the X chromosome received from the mother (The young boys receive the Y chromosome from the father.). This condition is a result of mutations in the dystrophin gene. Dystrophin is part of a protein complex within muscle cells that strengthens and protects muscle fibers during flexion and relaxation. Genetic abnormalities in dystrophin result in muscle cell death and accumulation of fibrotic, nonfunctional muscle tissue. Dystrophin is primarily present in skeletal and cardiac muscle, but it also exists in small amounts in nerve cells and brain tissue. 1 Duchenne muscular dystrophy is the most common and severe form of childhood muscular dystrophy, affecting one in every 3,500 boys. The disease is typically diagnosed between the ages of 2 and 5 years, with a delay in gross motor milestones. DMD normally presents with abnormal gait, calf hypertrophy, and difficulty rising from the floor. Independent ambulation is typically lost by age 10, resulting in nearly complete wheelchair dependency. More severe complications emerge after this phase, including scoliosis, weight loss, decreased respiratory reserve, pneumonia, and dilated cardiomyopathy. Death is likely to occur by the boy’s late teens or early twenties. 2 Corrective orthopedic surgery, such as corrective joint surgery, may be needed to improve function. Percutaneous muscle release surgery may relieve painful muscle and tendon contractures, which are commonly associated with DMD. 1 PT 100 Computer Library Project Citations 1. Eddy LL. Caring for Children with Special Healthcare Needs and their Families: A Handbook for Healthcare Professionals. Ames, Iowa: John Wiley & Sons, Inc., Publication; 2013. Book from Penn State Mont Alto Library. 2. Manzur A, Muntoni F. Diagnosis and new treatments in muscular dystrophies. Journal of Neurology, Neurosurgery & Psychiatry. July 2009; 80 (7):706-714. Online Journal article from CINAHL. 3. Long, Terry, Robertson, Terry. Foundations of Therapeutic Recreation. Champaign, IL: Human Kinetics; 2008. Book from another Penn State Library. 4. Markert, C. D., Ambrosio, F., Call, J. A. and Grange, R. W. Exercise and Duchenne muscular dystrophy: Toward evidence-based exercise prescription. Muscle & Nerve. 2011-04;43:464-478. Online article from PubMed. 5. Rose KJ, Burns J, Wheeler DM, North KN. Interventions for increasing ankle range of motion in patients with neuromuscular disease. Cochrane Database of Systematic Reviews 2010, Issue 2. Art. No.: CD006973. DOI: 10.1002/14651858.CD006973.pub2. Review from Cochrane Library. 6. Sackley C, Disler PB, Turner-Stokes L, Wade DT, Brittle N, Hoppitt T. Rehabilitation interventions for foot drop in neuromuscular disease. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD003908. DOI: 10.1002/14651858.CD003908.pub3. Review from Cochrane Library.