Indwelling Urinary Catheter Protocol
advertisement

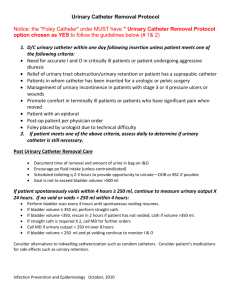
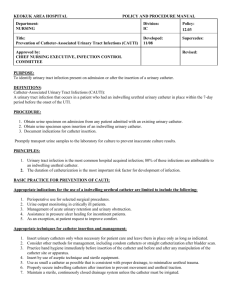
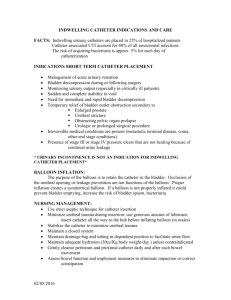
Title: Indwelling Urinary Catheter Protocol Protocol Saint Francis Hospital and Medical Center Mount Sinai Rehabilitation Hospital Saint Francis Medical Group, Inc. Saint Francis Care Medical Group, P.C. Asylum Hill Family Medicine Center, Inc. Saint Francis Behavioral Health Group, P.C. Saint Francis Emergency Medicine Group, P.C. Proponent Department Patient Care Number Level CLIN.0171 Category Published Date System Division Department Review Cycle Administrative Clinical HR EOC 12/28/2012 1 year 3 years PURPOSE To implement best practices to prevent catheter-associated urinary tract infections. SCOPE Clinicians responsible for ordering, inserting, maintaining and discontinuing indwelling urinary catheters. POLICY 1. Indwelling urinary catheters will be inserted by a licensed practitioner only when necessary with an Physician/APP (Advanced Practice Practitioner) order. 2. When ordering an indwelling urinary catheter, the physician or APP (Advanced Practice Practitioner) will document the necessity for the catheter by using the insertion criteria listed. 3. Clinicians inserting and maintaining a catheter will have knowledge of aseptic technique and procedures for catheter and drainage system maintenance. 4. Consideration will be given to alternatives to indwelling catheters, such as external drainage device or intermittent catheterization. 5. An assessment of catheter necessity will be performed and the catheter removed as soon as possible. 6. In the event of post operative urinary retention (POUR), bladder scanning will be performed and the results reported to the physician/APP. Intermittent catheterization will be considered. 7. If Physician/APP states the urinary catheter cannot be removed, the rationale for need for urinary catheter must be documented by the Physician/APP and RN. 8. A Physician/APP order for indwelling catheter removal is not needed when protocol removal criteria are met. POPULATION OR CLINICAL CONDITION Patient whose clinical condition warrants the insertion of an indwelling urinary catheter. PROTOCOL: Indwelling Urinary Catheter Protocol Date: 12/28/2012 Page 1 of 4 I. CAUTI PREVENTION BUNDLE-CRITERIA FOR INSERTION 1. Use of an indwelling urinary catheter is assessed using the following insertion criteria: a. Requires accurate monitoring of urine output in the hemodynamically unstable patient. Examples include (but not limited to): Severe hypotension Neurological impairment Multi-system trauma b. Requires management of acute urinary retention and urinary obstruction confirmed by clinical exam, bladder ultrasound, palpable urinary bladder and/or patient symptoms. c. Assistance in Stage III or IV pressure ulcer or wound healing in the incontinent patient unable to use alternative measures. d. Patient comfort during end-of-life care. e. Urinary catheters will be inserted in the operating room for selected surgical procedures: Expected duration of operation greater than or equal to 3 hours Expected intraperitoneal urologic, gynecologic, pelvic, colorectal dissection or extensive extraperitoneal anorectal dissection with or without anastomosis Critically ill patients requiring emergent surgery and in need of physiologic monitoring and volume resuscitation f. Physically deconditioned patient who experiences significant pain due to unstable fractures if unable to use alternative methods e.g. external drainage device, urinals, etc. II. INSERTION OF URINARY CATHETER 1. Urinary catheters will be inserted using aseptic technique. 2. Follow link for insertion of catheter in female a. Female b. Male 3. Document insertion date, time and initials in the medical record 4. Apply label with insertion date, time and initials to the drainage tubing 5. Provide patient and family education III. CAUTI PREVENTION BUNDLE-URINARY CATHETER MAINTENANCE 1. Maintain urinary catheters and closed system as outlined in attached procedures. http://procedures.lww.com/lnp/view.do?pId=5487&s=p&fromSearch=true&searchQuery=uri nary+catheters 2. Perform hand hygiene and use standard precautions prior to any urinary catheter care 3. Routine Maintenance includes the following a. Perineal care with hospital approved bath product b. Daily and as needed when soiled c. Catheter is cleaned from the perineum outward d. Prevent looping or kinking of drainage tube by using the linen clip e. Secure catheter to leg Indwelling Urinary Catheter Protocol Date: 12/28/2012 Page 2 of 4 2. 3. 4. 5. 6. 7. f. Drainage tubing is labeled with the insertion date, time and initials g. Maintain the drainage bag below the bladder with all activities h. Maintain a closed system i. Do not place the drainage bag on the floor Emptying bag at least once every 8 hours and when clinically indicated a. Separate/labeled graduate for each patient b. Label graduate with room number, patient initials & “Urine only” with permanent marker c. Avoid touching sides of the graduate with drainage spigot Clean sample port with chlorhexidine wipe for 15 seconds and let air dry prior to obtaining sample (Scrub the hub) a. Obtain urine specimens from indwelling urinary catheter using sterile technique to prevent catheter contamination. http://procedures.lww.com/lnp/view.do?pId=5381&s=p&fromSearch=true&searchQuery=uri nary+catheters Do not routinely clamp prior to removal Bladder scan first before irrigating if no urinary output (no routine irrigation) If system integrity becomes compromised, the entire system including catheter will be changed Use aseptic technique if system needs to be opened in order to change bag IV. CAUTI PREVENTION BUNDLE ONGOING NEEDS ASSESSMENT CRITERIA 1. Nurse will assess and document the need for an indwelling catheter every shift 2. If criteria is not met, the catheter will be removed per protocol V. CAUTI PREVENTION BUNDLE- CRITERIA FOR CATHETER REMOVAL 1. Nurse will consult the PHYSICIAN/APP before removing catheter if patient: a. Has gross hematuria b. Had extensive urologic, gynecologic, pelvic or colorectal surgery c. Is urology patient or Urology Service inserted urinary catheter 2. Nurse will remove indwelling urinary catheter without a Physician/APP order: a. Within 48 hours after insertion for post-operative patients b. When any single criteria listed below is met for non-surgical patients: A stable patient no longer requires frequent monitoring of urine output. No longer exhibits signs and symptoms of urinary retention or obstruction Note: If catheter was inserted due to a problem with mechanical obstruction, please communicate with the appropriate attending prior to removal. Pressure ulcer or wound not impacted by not using an indwelling catheter Physician/APP order specifies date and/or time of urinary catheter removal 3. If no exclusion factors are noted, the RN will discontinue the catheter and document date and time of removal and monitor urinary output every 8 hours x 24 hours. 4. If patient is unable to void within 6-8 hours or patient is incontinent, assess patient (clinical exam, palpable urinary bladder, bladder ultrasound, patient symptoms) to determine if straight catheterization is needed. a. Intermittent/straight catheterization is preferable to indwelling urethral or suprapubic catheters in patients with bladder emptying dysfunction. Frequency of straight catheterization is determined by nursing assessment and patient comfort. Indwelling Urinary Catheter Protocol Date: 12/28/2012 Page 3 of 4 VI. CAUTI PREVENTION BUNDLE CRITERIA FOR CONTINUED CATHETER USE 1. The urinary catheter may be continued if one of the following criteria is met: a. Requires accurate monitoring of urine output in the hemodynamically unstable patient. b. Management of acute urinary retention and urinary obstruction c. Assistance in Stage III or IV pressure ulcer or wound healing for incontinent patient unable to use alternative measures d. Comfort during end-of-life care e. Meets criteria for peri-operative use for selected surgical procedures. f. Physically deconditioned patient who experiences significant pain due to unstable fractures if unable to use alternative methods e.g. condom catheters, urinals, etc. 2. If there is a need to continue use of the indwelling urinary catheter, the rationale for continuation must be documented. REFERENCES: SHEA-IDSA – Society for Healthcare epidemiology of America/Infectious Disease of America CDC – Centers for Disease Control ACS- NSQIP Best Practice for CAUTI Prevention NHS – National Health Service IHI-How to Guide: Prevent Catheter- Associated Urinary Tract Infections HICPAC-Guideline for Prevention of Catheter-Associated Urinary Tract Infections 2009 CROSS REFERENCES: Applicable Lippincott Procedures REVIEWED BY: CAUTI Committee 12/12 APPROVED BY: See policy for required approval(s). Title: Rebecca L. Burke, RN, MS, NEA-BC SVP, Clinical Services, Chief Nursing Officer Rolf Knoll, M.D. Senior Vice President, Medical Affairs Chief Medical Officer Date: 12/28/2012 Committee(s), if applicable: Date: 12/18/2012 REPLACES: Foley Catheter Associate UTI Prevention Guideline – CAUTI Bundle 12/2010 KEY CHANGES: Addition of Urinary Catheter Maintenance; Specific criteria for insertion and continuation of indwelling catheter; Need assessment Indwelling Urinary Catheter Protocol Date: 12/28/2012 Page 4 of 4