Sample Policy & Procedure for CAUTI
advertisement

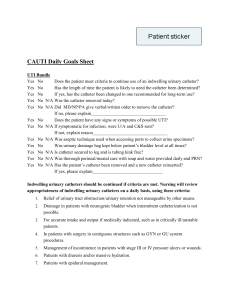
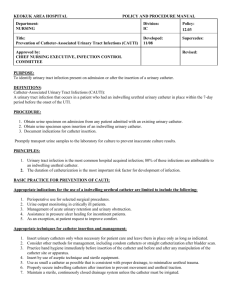
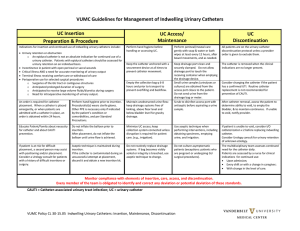
LIFECARE MEDICAL CENTER – POLICY & PROCEDURE ----------------------------------------------------------------------------------------------------------------------------DEPARTMENT: Facility-wide SUBJECT: CAUTI Prevention (Catheter Associated Urinary Tract Infection) ----------------------------------------------------------------------------------------------------------------------------PREPARED BY: J. Hirst, RN, IP APPROVED BY: PPC, 4/10; Medical Staff, 5/10 PURPOSE: Limit indwelling urethral catheter use to patients/clients/residents with appropriate indications/criteria. POLICY: LifeCare Medical Center will implement Best Practices for Prevention of CAUTI using evidence-based guidelines to prevent and eliminate these infections and comply with ZERO tolerance for preventable HAI’s. BACKGROUND: As the most common healthcare-associated infection (HAI), catheter-associated urinary tract infections (CAUTIs) dramatically impact the lives of tens of thousands of patients each year. Foley catheters can cause increased infections, increased length of stay, increased cost, increased patient discomfort and increased antibiotic usage. Literature reports numerous organizations have implemented successful strategies to reduce CAUTI. This work has resulted in recommendations for best practices. GUIDELINES: Indications/criteria for the use of indwelling urinary catheters: Perioperative use for surgical procedures (eg. surgeries involving the Genitourinary Tract, anticipated prolonged surgery, operative patients with urinary incontinence, need for intraoperative hemodynamic monitoring, patients to receive large volume diuretics during surgery) may be needed short term post-op (usually removed within 24-48 hours). Urine output monitoring in critically ill patients Management of acute urinary retention and urinary obstruction Assistance in pressure ulcer healing for incontinence Hospice - comfort or palliative care (if patient requests) Patient requiring prolonged immobilization (eg. Potentially unstable thoracic or lumbar spine, multiple traumatic injuries such as pelvic fractures) Best Practices: Do not use the indwelling catheter unless appropriate indications/ criteria are met Leave catheter in only as long as indications/criteria persist. Use condom catheters or intermittent catheterization in appropriate patients Use Bladder scanner/ultrasound to assess urine volume to reduce unnecessary catheterization Use of as small of a catheter as possible to minimize bladder neck and urethral trauma Use aseptic technique and sterile equipment for insertion Secure catheters to prevent movement and urethral traction 1 Hand hygiene immediately before donning gloves for insertion and before and after any manipulation of the catheter site or apparatus Maintain sterile closed system below the level of the bladder including during transport and ambulation Maintain unobstructed urine flow, tubing free of kinks and dependent loops In Acute Care do not disconnect catheter from collection bag unless the catheter must be irrigated Empty the collection bag regularly using a clean container for each patient; avoid splashing, and preventing contact of the drainage spigot with the nonsterile collection container In Acute Care obtain urine sample through the sampling port using disinfectant to clean the port prior to obtaining the sample In Acute Care for larger urine samples use aseptic technique to remove sample from drainage bag Use aseptic technique if the drainage bag needs replacement Hand hygiene prior to donning gloves to remove catheters Catheter care daily and PRN- clean meatal area using routine hygiene procedure Required documentation in the medical record includes: Indications for catheter insertion Date and time of insertion Individual’s name who inserted the catheter Date and time of catheter removal Time and amount of first void after removal Assessing catheter necessity: Review of urinary catheters for Long Term Care residents and Home Health Care clients will be done on a regular basis. When doing Acute Care inpatient daily rounds, physicians and nurses will review patients with urinary catheters to ascertain continuing necessity. If it is noted catheter use needs to be addressed the nurse needs to contact the physician of this. REFERENCES: 2008 APIC Guide to the Elimination of Catheter-Associated Urinary Tract Infections (CAUTIs) HICPAC (Healthcare Infection Control Practices Advisory Committee) Guideline for Prevention of Catheter-Associated Urinary Tract Infections 2009 Joint Commission Standard 02.22.01 PP/DRAFT/infection control/CAUTI 6-12 Original Date: 4/10 Reviewed: 6/12 Revised: 6/12 COPIES ROUTED TO: Long Term Care Home Care Acute Care 2