3. SI management in 2010/11 - Cambridgeshire and Peterborough
advertisement

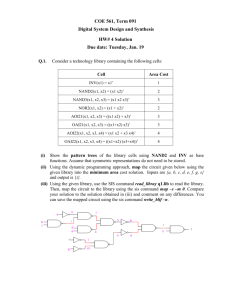
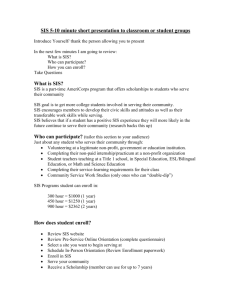
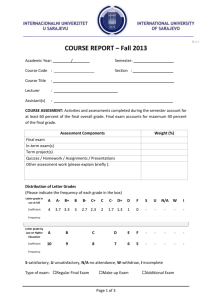
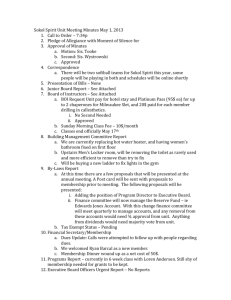
Annual Report on Management of Serious Incidents - 1 April 10 to 31 March 11 Wendy Lefort, Quality & Governance Manager, August 2011 Contents 1. Introduction ............................................................................................................................1 2. National Patient Safety Agency framework .............................................................................2 3. SI management in 2010/11 ....................................................................................................2 4. Analysis of SIs in 2010/11 ......................................................................................................4 5. Never Events..........................................................................................................................5 6. Providers reporting SIs ...........................................................................................................5 7. Learning from SIs ...................................................................................................................6 8. Dissemination of learning .......................................................................................................7 10. Summary................................................................................................................................8 11. Recommendations .................................................................................................................9 Appendix 1 – NPSA changes to SI grades .................................................................................... 10 Appendix 2 – Targets for NHSC/P SI monitoring system objectives .............................................. 10 Appendix 3 – Overall SI activity in 2010/11.................................................................................... 11 Appendix 4 – List of Never Events ................................................................................................. 13 Appendix 5 – SI analysis by provider ............................................................................................. 14 Appendix 6 – Examples of action taken by providers following SI investigation ............................. 21 Appendix 7 – Glossary .................................................................................................................. 22 1. Introduction NHS Cambridgeshire (NHSC) and NHS Peterborough (NHSP) (the PCT) have a responsibility for commissioning services that deliver safe and high quality healthcare for the population of Cambridgeshire and Peterborough. As part of this role, the PCT holds providers to account through a clinical quality review (CQR) process and other governance mechanisms. Providers are required to provide evidence as assurance that the trust is meeting the quality indicators set out in the contract with the PCT. The reporting and investigation of Serious Incidents (SIs), and taking forward improvements from learning from these incidents is a significant part of the quality and patient safety agenda of each provider trust. Using investigation and learning from SIs is a proven mechanism to drive improvement in patient care. Provider organisations have both a statutory and a contractual duty to have robust incident and SI management systems that allow open and thorough reporting, investigation and learning. The management of SIs includes not only identification, reporting and investigation of each incident, but also implementation of any recommendations following investigation, assurance that implementation has led to improvements in care, dissemination of learning to prevent recurrence, and thematic review to drive systemic change. NHSC/P SI Annual Report 10/11 Page 1 of 23 August 2011 2. National Patient Safety Agency framework The National Patient Safety Agency (NPSA) ‘National Framework for Reporting and Learning from Serious Incidents Requiring Investigation’ came into force in April 2010. The framework formalised the SI management requirements and provided national measurable indicators for timeliness of SI reporting. These are used as the basis of the contract quality indicators between the PCT and provider. The framework also clarified roles and responsibilities for SI management and redefined SI definitions and grades. Further details of the new grading system are given in Appendix 1. The PCT and its provider services have been working to this framework throughout 2010/11. 3. SI management in 2010/11 As part of the commissioning role of monitoring quality and patient safety in commissioned services, the PCT has responsibility to scrutinise the providers’ management of SIs. This report summarises the SIs monitored by the PCT during 2010/11, giving comparison with the previous year where appropriate. At the start of 2010/11 the commissioner approach to monitoring provider SI management was supportive, with providers allowed to develop their SI systems in line with the NPSA framework, and timescales for reporting not rigorously enforced. The PCT had a range of mechanisms in place to monitor the management of provider SIs including: Assessment of initial SI reports, updates on immediate action taken, final investigation reports and action plan updates Feedback on SI reports, including requirement for additional investigation Follow-up on areas of concern. For example the NHSC Associate Medical Directors carried out an audit of incident reporting at Papworth following concern about the low number of SIs reported. This provided assurance that a comprehensive system is in place to assess, review and reflect on incidents and determine those which meet the definition of SIs. Co-ordination of multiorganisational SIs, including review of individual organisation investigations and oversight of combined report and cross-boundary action plan implementation At the start of 2011, the PCT’s holding to account approach to provider quality indicators was significantly strengthened with the use of contract levers to address poor performance. A review of SI timeliness and quality of reporting showed that the supportive approach had not achieved the necessary outcomes. A more performance based approach was introduced to be in line with the overall approach to quality indicator monitoring. NHSC/P SI Annual Report 10/11 Page 2 of 23 August 2011 Procedures introduced include: A regular flagging system to clarify outstanding reporting requirements to providers Increased PCT senior clinician and management involvement to ensure relevant issues from SIs are escalated. Thus the importance of prompt and robust investigation leading to improvements in care is modelled by the PCT and can be promoted to providers with the aim of embedded in their culture. A PCT cluster escalation policy which ensures any concerns regarding SIs and SI management are escalated to the appropriate level and drive remedial action if required A regular PCT SI Quality Assurance meeting to involve both clinical and operational staff, reviewing all new SIs, those awaiting closure and all SIs that have been open for more than 6 months Development of the SI database to include additional performance information about timeliness of reporting and response to queries The early results from the procedures put in place show some improvement in timeliness of reporting, and has lead to an increase in SIs closed following completion of action plans. The SHA positively recognise the improvements made to date. Providers that have failed to show expected improvements are currently subject to contract escalations. The PCT is monitoring progress and have produced a range of metrics to measure process. However, there is still concern about the outcome of SIs, with the quality of final reports and action plans inconsistent, and a lack of thematic review to support further learning. To address these gaps, further procedures are proposed, as follows: Additional quality assurance for final report review to maximise learning from the SI, and to identify any themes across other SIs. This will be supported by the SI Quality Assurance meeting. Requirement for more regular thematic review including areas of concern and other issues raised at SI Quality Assurance meetings, CQRs and other sources Triangulation of SI investigation and learning with any improvement plans in place for providers. For example a Care Quality Commission concern about staffing would prompt a more in-depth review of staffing issues in the SI investigation. Review of outcome evidence, including clinical audit, to demonstrate whether required improvements following an SI are being embedded at service level Lowering of thresholds for SI reporting where there are significant concerns with provider performance to ensure robust investigation of a wider range of incidents that will inform the improvement plans of the provider A set of outcomes for the PCT SI monitoring system has been agreed which will give measurable evidence of the effectiveness of the changes put in place. These include: A reduction in delayed SI reporting which will result in prompter implementation of actions from SI learning NHSC/P SI Annual Report 10/11 Page 3 of 23 August 2011 A reduction in the number of SIs where the PCT has to ask additional questions following review of initial and final reports and action plans, indicating more robust reporting with provider ownership Following thematic review and learning from similar SIs, a reduction in SIs in areas under review or a reduction in the common root causes in these SIs Targets for these outcomes are given in Appendix 2. 4. Analysis of SIs in 2010/11 The significant changes in overall SI activity are summarised below. Further details are given in Appendix 3. Please note that there are limited statistics available for NHSP for 2010/11 due to different data collection systems and limited capacity. There was a substantial reduction in SIs related to infection control (from 17 in 2009/10 to 3 in 2010/11 for NHSC). This is due to the effectiveness of improvements in infection control systems in NHS providers leading to a reduction in the incidence of MRSA and C difficle infections. The last three months of the 2010/11 saw a significant increase in the reporting of grade 3 and grade 4 pressure ulcers. This was due to work put in place by trusts to stress the importance of reporting and investigating these incidents, highlighted by national and local focus on pressure ulcers in quality indicators and initiatives. A programme of work aimed to reduce the incidence of avoidable pressure ulcers has started for 2011/12. This includes streamlined reporting systems using a template designed together with providers, a county wider pressure ulcer group to share learning across the health economy, and inclusion of pressure ulcer targets in provider’s Commissioning for Quality and Innovation (CQUIN) frameworks. The number of suicides / possible suicides increased from 16 in 2009/10 to 28 in 2011/12 (NHSC figures). The PCT have been working closely with the mental health provider (Cambridge & Peterborough Foundation Trust (CPFT)) to address the root causes identified for SIs relating to suicide. The quality of risk assessments and care planning was highlighted as a theme in the NHSC review of final reports relating to suicide. CPFT have put actions put in place as part of the suicide prevention work to address these areas. Actions taken to date by CPFT include: o Use of a Global Trigger Tool to identify patients at risk o Improvement of risk assessment training for all clinical staff o Clinical audit of clinical risk assessment and evaluation of care plans for inpatients The trust has rolled out a refresher training programme for management of depression, and established a joint Suicide Prevention Group linking with GPs to ensure appropriate risk assessment at all stages. NHSC/P SI Annual Report 10/11 Page 4 of 23 August 2011 5. Never Events The Department of Health defined a list of eight Never Events in 2010. These are serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented. This list was increased to 25 in April 2011. These are given in Appendix 4. Never Events must always be reported as grade 2 SIs. They attract more in-depth management and review, and providers will be rated as Red whilst they have an investigation ongoing for any Never Event. There is also a financial penalty for the provider. There was one Never Event reported in NHSC and NHSP in 2010/11. This incident has been investigated both internally and though external scrutiny, and the recommendations of the investigation are being implemented. The CQR receives regular updates to ensure the learning from this minimises the likelihood of recurrence. 6. Providers reporting SIs There are four main providers reporting SIs to NHSC. These are: Two acute trusts, Cambridge University Hospital Foundation Trust (CUH) and Hinchingbrooke Healthcare Trust (HHCT) One mental health trust, Cambridgeshire & Peterborough Foundation Trust (CPFT) One community provider, Cambridge Community Services (CCS) Other trusts that report SIs to NHSC include: Out-of-hours service, Urgent Care Cambridge (UCC) Papworth Hospital NHS Foundation Trust – Papworth is jointly commissioned by NHSC and the East of England Specialised Commissioning Group (which commissions specialised health services on behalf of all EoE PCTs). When an SI occurs at Papworth, the route for reporting is determined by the service where the incident occurred. HMP Littlehey and HMP Whitemoor EoE Ambulance NHS Trust - the trust reports SIs that relate to NHSC patients or services NHSC SIs - SIs that relate to independent contractors, or involve multiple agencies, are reported and investigated by NHSC Analysis of SIs reported by providers is given in Appendix 5. NHSC/P SI Annual Report 10/11 Page 5 of 23 August 2011 The following providers reported SIs to NHSP in 2010-2011: One acute trust, Peterborough and Stamford Hospital Foundation trust (PSHFT)) One mental health trust, Cambridgeshire & Peterborough Foundation Trust (CPFT) One community provider, Peterborough Community Services (PCS) Other trusts that report SIs to NHSP include: Out-of-hours service, Peterborough HMP Peterborough (Kalyx) NHSP SIs - SIs that relate to independent contractors, or involve multiple agencies, are reported and investigated by NHSP 7. Learning from SIs The PCT reviews SI final reports to ensure all relevant aspects of the SI have been investigated and recommendations follow from the investigation findings. This process is being strengthened to challenge providers to consider further areas of learning and how learning can be embedded. Review of final reports in 2010/11 show investigations highlight the importance of having clear policies and procedures, and training in place to support staff. Several SIs raise the importance of good interaction and communication between staff, and of ensuring staff are engaged and aware of their accountability in all areas of work. The issue of poor documentation remains a significant contributing factor to many SIs. Provider resource issues and staffing levels were only identified as factors in a small percentage of SIs. However, this will need careful monitoring as the NHS moves into a period of significant financial pressures and greater levels of staff in transition as a result of NHS reform. The main root causes identified from SIs in 2011/12 are similar to those recorded in 2009/10. The PCT is working with providers to focus on systems that address these generic causes. However, these root causes are likely to remain the main concerns, as they reflect situations where systems were not used or did not support staff adequately. One of the most important aspects of SI management is ensuring prompt implementation of any changes resulting from the SI investigation. The PCT monitors the implementation of recommendations from SI investigations to ensure changes are made to improve care. Some of the changes made by trusts resulting from learning from SIs are given in Appendix 6. NHSC and NHSP will be working with providers to address the next step of whether changes have led to improvement, using clinical audit and other quality assurance processes. The timeliness of actions will also be addressed to ensure that actions are implemented without inappropriate delay. NHSC/P SI Annual Report 10/11 Page 6 of 23 August 2011 8. Dissemination of learning NHSC and NHSP disseminate findings from SIs and thematic reviews across the health economy where there is appropriate learning. This is done via: Targeted newsletters, such as the Clinical Governance newsletter sent to all GPs, dentists and optometrists Learning events, such as the countywide SI meeting, or at specific groups such as the Dental Audit meeting Development of SI reporting requirements to include clinician leadership and involvement of patients and families Robust monitoring at CQRs between NHSC, NHSP and providers to ensure compliance with a range of quality indicators, including SI management. CQUIN and Quality Account negotiations to ensure improvement is rewarded where needed and priorities for improvement take on board recent SI learning Intelligence shared across the health economy at the SI learning meetings includes: Clinical leaders throughout the NHS must advocate and lead the necessary changes There must be significant focus on procedures to support staff in exceptional situations such as the swine-flu epidemic Clarification of process where incidents result from poor practice/actions of independent agencies The need for a joined-up approach to ensure appropriate information is available at each stage of the patient’s journey To further strength the dissemination of learning, NHSC and NHSP will require providers to provide a summary of learning from SIs that can be shared across the health economy by the PCT, and to use their networks to disseminate learning widely with their peer organisations. 9. Timeliness of SI reporting and investigation The timeliness of SI reporting is an indicator of both level of clinical engagement, ownership and leadership, and the capacity and capability of the trust in carrying out root cause analysis. Prompt reporting and investigation leads to remedial action and action for improvement being implemented as soon as possible. Lack of ownership and poor engagement lowers commissioner confidence that provider organisations have a robust culture in place to maintain resilience for quality and patient safety in transition. The table below shows that timeliness of final reports has improved slightly during 2010/12 but remains well below the targets set for reporting by the NPSA framework and the NHSC/P SI procedure. All providers remain non-compliant with the requirement for providers to complete grade 1 investigations within 9 weeks of reporting, unless there are valid reasons for delay. The outcome of an investigation may be delayed by police involvement or the need for an inquest. However lack of capability and capacity will no longer be accepted as a valid reason for delay. NHSC/P SI Annual Report 10/11 Page 7 of 23 August 2011 Number of weeks taken for SI investigation Weeks between date # of reporting and final 2010/11 report received No. (%) of SIs Within reporting timescales 9 or less weeks 23 20% Outside reporting timescales 10 – 19 47 40% 20 – 29 25 21% 30 – 39 7 6% 40 – 49 5 4% 50 – 59 4 3% More than 59 7 6% Median (weeks) Maximum (weeks) 16 128 2009/10 No. (%) of SIs 16 13% 19 25 14 16 16 14 16% 21% 12% 13% 13% 12% 30 138 The NPSA framework sets out timescales for reporting that cover not only final reports, but also other deadlines as set out below. These timescales have been set to allow providers time to complete full investigations, whilst ensuring immediate remedial action is identified where necessary and improvements in care implemented as soon as possible. Type of Report Required Timescales Initial reports Initial updates 2 working days from date of incident 7 working days from date SI received for level 1 3 working days for level 2 and Never Events 9 weeks from date SI received for grade 1 12 weeks for grade 2 / Never Event 4 weeks after last action on action plan Final reports Action plans Because of the importance of learning from SIs in a timely way, the PCT have put in place mechanisms to highlight and monitor any delay in reporting. Regular performance information is addressed in the CQRs and contract penalties will be used to hold to account providers who consistently miss the deadlines for SI reporting. 10. Summary The introduction of the NPSA framework for management of SIs in April 2010 has lead to development of more robust systems in providers. This has been coupled with increased monitoring by NHSC and NHSP to ensure timely reporting and high quality final reports and action plans. There was a substantial reduction in SIs related to infection control, reflecting the effectiveness of improvements in infection control systems in NHS providers. The last three months of the 2010/11 saw a significant increase in the reporting of grade 3 and grade 4 pressure ulcers. This was due to work put in place by trusts to stress the importance of reporting and investigating these incidents, highlighted NHSC/P SI Annual Report 10/11 Page 8 of 23 August 2011 by national and local focus on pressure ulcers in quality indicators and initiatives. Providers have targets to eliminate all avoidable pressure ulcers and this will be monitored during 2011/12. The number of suicides increased during 2011/12. The quality of risk assessments and care planning was highlighted as a theme in the NHSC review of final reports relating to suicide. CPFT have put actions put in place as part of the suicide prevention work to address these areas. The information available for analysis of SI management in 2010/11 was limited by the data collected on the SI database at the beginning of the period. During 2010/11 the expectation for providers to have much more robust SI management systems has necessitated a significant increase in data collected. This will be available to measure both provider and commissioner performance during 2011/12. A range of mechanisms has been put in place to strengthen the commissioner’s role in monitoring SI management of providers. The effectiveness of these systems will be measured against a set of objectives for the PCT. NHSC and NHSP will continue to hold providers to account where they do not comply with the NHSC/P SI procedure. 11. Recommendations 1. Embed the new mechanisms put in place by the PCT to monitor provider SI management, and monitor their effectiveness using measurable objectives for the NHSC/P SI monitoring systems: Reduction in delayed SI reporting Reduction in the number of SIs where the PCT has to ask additional questions following review of initial and final reports and action plans Reduction in pressure ulcers and suicide SIs, and SIs in other areas highlighted by thematic review where overarching actions are put in place to address systems problems in these areas 2. Strengthen the review of action plan monitoring, ensuring prompt implementation of recommendations, and use of clinical audit and evaluation to ensure changes have led to improvements. 3. Hold providers to account against the NHSC/P SI procedure for SI management, using contract levers where necessary to ensure reporting organisations give timely updates and final reports of the investigation into the SI, and follow up recommendations and implement action plans in order to improve care. 4. Ensure the learning from SIs is disseminated widely and appropriately, both by providers and the PCT. Providers will be required to provide a summary of learning from SIs that can be shared across the health economy by the PCT, and to use their networks to disseminate learning widely with their peer organisations. NHSC/P SI Annual Report 10/11 Page 9 of 23 August 2011 Appendix 1 – NPSA changes to SI grades The NPSA framework sets out a revised grading system for SIs with grades 1 or 2 allocated to incidents. Grade 1 incidents require investigation using NPSA root cause analysis (RCA). Grade 2 incidents require closer monitoring and involvement by the PCT and/or NHS EoE (the local Strategic Health Authority (SHA)) and may require an independent investigation to complete the RCA. Providers must also notify the PCT about any incident where it is unclear initially if the incident meets the definition of an SI. These notifications are given a grade 0. This gives the provider the chance to investigate further and determine if the incident does meet the definition of an SI. If not, the incident is downgraded and is not subject to the robust investigation required for an SI. However, investigation will still take place within the provider organisations as part of their incident reporting system. Appendix 2 – Targets for NHSC/P SI monitoring system objectives Objective Reduction in delayed SI reporting Type of NPSA timescale Target report Initial 2 working days from date of 80% of SIs reported to reports incident timescale, or valid reason for delay in reporting agreed Initial 7 working days from date 80% of SIs reported to updates SI received for level 1 timescale, or valid reason for 3 working days for level 2 delay in reporting agreed and Never Events Final 9 weeks from date SI 50% of SIs reported to reports received for grade 1 timescale, or valid reason for 12 weeks for grade 2 / delay in reporting agreed Never Event Action 4 weeks after last action on 75% of action plans completed plans action plan to timescale, or valid reason for delay in reporting agreed Current performance Estimate 40% (2010/11) Estimate 40% (2010/11) 20% (2010/11 NHSC) NA Objective Reduction in number of SIs where the PCT has to ask additional questions Target Current performance Comments 2011/12 – 50% 26% (Jan – June 2012) This should increase initially as the PCT puts in 2012/13 – 20% place a more robust peer review system for reports Objective Reduction in number of Pressure ulcer and suicide SIs, and any other areas highlighted by thematic review Area Target Current performance Pressure ulcers 35 (Jan – June 2012) 53 (Jan – June 2011) Suicides 22 (April 2011 – Mar 2012) 28 (April 2010 – Mar 2011 NHSC) Other targets will be set as appropriate following thematic review Objective Improvement in timeliness of review and feedback for final reports Target Current performance Comment 95% Feedback within 20 days for all SIs 83% (Jan – June 2011) NPSA target NHSC/P SI Annual Report 10/11 Page 10 of 23 August 2011 Appendix 3 – Overall SI activity in 2010/11 Number of SIs The number of SIs monitored by NHSC between 1 April 2010 and 31 March 2011 is given below. The changes to the monitoring of SIs has resulted in more detailed information being available for 2010/11 than for 2009/10. Status 2010/11 2009/10 SIs reported during period 110 SIs occurring in the period (reported as at end July 2011) 122 SI investigations completed during period 100 SI action plans completed during the period - SI closed 47 Not recorded 101 Not recorded SIs open at end of period 89 Not recorded 120 The number of SIs occurring is greater than those reported due mainly to the late reporting of several pressure ulcer SIs. This delay is being addressed with the provider in question. Of the 101 SIs open at the end of 2010/11, 47 were being investigated. For the remaining 54, recommendations have been approved and the trusts are implementing the action plans. The number of SIs monitored by NHSP between 1 April 2010 to 31 March 2011 is given below. Status SIs reported during period 2010/11 2009/10 57 26 Month of reporting The month of reporting for NHSC SIs is shown in the graph overleaf. This shows that SI reporting reduced during the first part of the year, and then increased over the last six months. Pressure ulcer reporting increased significantly in the first three months of 2011, with the increase in other areas spread across the NPSA categories. NHSC/P SI Annual Report 10/11 Page 11 of 23 August 2011 All NHSC SIs reported - 1 April 2010 to 31 March 2011 (with 2009/10 figures for comparison) 2009/10 2010/11 20 Number of SIs reported 15 10 5 0 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 SI categories Each SIs is classified under one of the NPSA defined categories. The table below shows the categories where 5 or more SIs were reported to NHSC in 2010/11, or where there have been significant changes from 2009/10. Category 2010/11 2009/10 Suicide / Possible Suicide 28 16 Clinical Assessment & Treatment 25 21 Pressure ulcer 9 0 Infection Control 3 17 Information 7 10 The number of NHSC SIs for each grade for 2010/11 are given below. The levels from 2009/10 are also given although these are not directly comparable. Grade 1 2 Total 2010/11 89 21 110 Level 1 and 2 3 Total 2009/10 54 35 89 As this was a new requirement under the NPSA framework, there was some variation in interpretation between providers, with some trusts not reporting any grade 0 SIs and another reporting 12, including 6 unexpected deaths and 4 missing persons. This discrepancy has now been addressed and the requirements agreed with providers. After review, 23 incidents reported as grade 0 during 2010/11 did not meet the definition of a SI and these were downgraded, and are not included in the analysis for this report. There were two grade 0 SIs awaiting assessment as at 31 March 2011. NHSC/P SI Annual Report 10/11 Page 12 of 23 August 2011 Appendix 4 – List of Never Events Never events are defined as ‘serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented by healthcare providers’. To be a “never event”, an incident must fulfil the following criteria; The incident has clear potential for or has caused severe harm/death. There is evidence of occurrence in the past (i.e. it is a known source of risk). There is existing national guidance and/or national safety recommendations on how the event can be prevented and support for implementation. The event is largely preventable if the guidance is implemented. Occurrence can be easily defined, identified and continually measured. The following list shows the events from the original list, and those that have been added for 2011/12. 1. Wrong site surgery (existing) 2. Wrong implant/prosthesis (new) 3. Retained foreign object post-operation (existing) 4. Wrongly prepared high-risk injectable medication (new) 5. Maladministration of potassium-containing solutions (modified) 6. Wrong route administration of chemotherapy (existing) 7. Wrong route administration of oral/enteral treatment (new) 8. Intravenous administration of epidural medication (new) 9. Maladministration of Insulin (new) 10. Overdose of midazolam during conscious sedation (new) 11. Opioid overdose of an opioid-naïve patient (new) 12. Inappropriate administration of daily oral methotrexate (new) 13. Suicide using non-collapsible rails (existing) 14. Escape of a transferred prisoner (existing) 15. Falls from unrestricted windows (new) 16. Entrapment in bedrails (new) 17. Transfusion of ABO-incompatible blood components (new) 18. Transplantation of ABO or HLA-incompatible Organs (new) 19. Misplaced naso- or oro-gastric tubes (modified) 20. Wrong gas administered (new) 21. Failure to monitor and respond to oxygen saturation (new) 22. Air embolism (new) 23. Misidentification of patients (new) 24. Severe scalding of patients (new) 25. Maternal death due to post partum haemorrhage after elective Caesarean section (modified) NHSC/P SI Annual Report 10/11 Page 13 of 23 August 2011 Appendix 5 – SI analysis by provider NHS Cambridgeshire The number of SIs by reporting organisation for 1 April 2010 to 31 March 2011 is given below. This excludes any grade 0 SIs which are subsequently downgraded. Organisation SIs reported during period SIs occurring during period SI investigations completed during period SI action plans completed during period CUH 28 25 25 HHCT 17 19 CPFT 31 CCS Open SIs as at 31 March 2011 SIs being investigated Action plans being implemented 13 15 13 22 7 4 17 30 29 9 10 21 13 27 5 5 9 1 UCC 4 4 4 0 0 4 Prisons 2 2 1 2 1 0 EoE Ambulance 4 4 7 7 1 0 Papworth 1 3 1 0 0 1 NHSC 10 8 6 4 7 2 Total 110 122 100 47 47 54 The table shows a difference between the number of SIs reported and the number occurring during 2010/11. There can be a significant delay in an incident occurring and it being reported to the PCT. For example, there may be an inquest for a patient who appears to have died of natural causes (which would not be reported as an SI). The inquest may determine the death was not due to natural causes and an SI would then be raised. However, with the increase in pressure ulcers, some trusts have collected these SIs and not sent in a timely manner. The database has been extended to allow recording of acceptable delays, and providers will be held to account where the reason for delay in reporting is not valid. Further analysis of SIs reported in 2010/11 for NHSC’s major providers is given in the following pages. NHSC/P SI Annual Report 10/11 Page 14 of 23 August 2011 Cambridge University Hospitals NHS Foundation Trust The categories of CUH SIs are shown below: Category Clinical Assessment & Treatment Categories relating to patient care Other Number of SIs 12 11 5 There were no themes identified regarding the type or location of SIs reported by CUH. SIs categorised as relating to Clinical Assessment & Treatment covered a range of specialities within the Trust and the root causes included delay in escalation, poor planning of care and treatment, and lack of communication and documentation. The three pressure ulcers were all reported in the first quarter of 2011. The monthly reporting pattern for CUH is given below. CUH SIs reported - 1 April 2010 to 31 March 2011 7 6 Number of SIs reported 5 4 3 2 1 0 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Number of weeks taken for SI investigation % final reports completed within 9 weeks or less Median (weeks) Maximum (weeks) NHSC/P SI Annual Report 10/11 Page 15 of 23 30% 18 86 August 2011 Cambridgeshire Community Services The categories of CCS SIs are shown below: Category Pressure ulcer Categories relating to patient care Other Number of SIs 5 5 less than 5 Five pressure ulcer SIs were reported in the first quarter of 2011, following a campaign to increase awareness of the requirement to report and investigate such incidents. CCS were part of the multi-disciplinary team reviewing the end-of-life pathway across acute, primary and community care. The SI identified poor quality information available for families and carers of terminally ill patients, and CCS is working with other organisations to produce a more joined-up and accessible information pack. CCS staff frequently visit nursing and residential homes to care for patients and may identify SIs within these homes, particularly in relation to safeguarding of vulnerable adults. Trust staff report these incidents and CCS have a role to ensure the home takes action to address any safeguarding concerns. The monthly reporting pattern for CCS is given below. CCS SIs reported - 1 April 2010 to 31 March 2011 7 6 Number of SIs reported 5 4 3 2 1 0 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Number of weeks taken for SI investigation % final reports completed within 9 weeks or less Median (weeks) Maximum (weeks) NHSC/P SI Annual Report 10/11 Page 16 of 23 0% 15.5 30 August 2011 Cambridge and Peterborough NHS Foundation Trust The categories of CPFT SIs are shown below: Category Suicide / possible suicide Unexpected death (subsequently downgraded from SI) Other Number of SIs 20 8 less than 5 The quality of risk assessments and care planning was highlighted as a theme in the NHSC review of final reports relating to suicide. CPFT have put actions put in place as part of the suicide prevention work to address these areas. CPFT also plan to establish a joint Suicide Prevention Group linking with GPs to ensure appropriate risk assessment at all stages. CPFT used the grade 0 option for reporting 8 unexpected deaths during 2010/11. These subsequently were determined to be from natural causes. The monthly reporting pattern for CPFT is given below. CPFT NHSC SIs reported - 1 April 2010 to 31 March 2011 7 6 Number of SIs reported 5 4 3 2 1 0 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Number of weeks taken for SI investigation % final reports completed within 9 weeks or less Median (weeks) Maximum (weeks) NHSC/P SI Annual Report 10/11 Page 17 of 23 0% 21 128 August 2011 Hinchingbrooke Healthcare NHS Trust The categories of HHCT SIs are shown below: Category Number of SIs Clinical Assessment & Treatment 9 Categories relating to patient care 6 Other less than 5 HHCT had a number of SIs involving colorectal cancer surgery. NHSC requested assurance that this did not show professional or systemic concern which may not have been highlighted by individual reports. HHCT had already commissioned an independent external review, the recommendations of which are being followed through. HHCT carried out an audit of all colorectal operations that had been completed over the past three years. There were no other themes identified regarding the type or location of SIs reported by HHCT. SIs categorised as relating to Clinical Assessment & Treatment cover a range of specialities within the Trust and the root causes include issues with clinical engagement, lack of awareness of guidelines, and lack of communication. HHCT reported one Never Event during 2010/11 relating to a retained instrument. The monthly reporting pattern for HHCT is given below. HHCT SIs reported - 1 April 2010 to 31 March 2011 7 6 Number of SIs reported 5 4 3 2 1 0 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Number of weeks taken for SI investigation % final reports completed within 9 weeks or less Median (weeks) Maximum (weeks) NHSC/P SI Annual Report 10/11 Page 18 of 23 42% 12.5 27 August 2011 NHS Peterborough The number of SIs by reporting organisation for 1 April 2010 to 31 March 2011 is given below: Organisation Open SIs as at 1 April 2011 SIs being Action plans investigated being implemented SIs reported during period SIs closed during period PSHFT 12 3 17 2 PCS 7 3 13 3 CPFT 8 8 16 0 5 2 9 2 1 0 1 0 0 0 1 1 33 16 57 8 NHS Peterborough HMP Peterborough Specialist Commissionin g Total Intelligence from each provider has not been presented in this report. However, the following process are now in place to ensure complete and robust information is available for 2011/12: Capacity for managing NHSP SIs has been identified in the Integrated Quality and Governance team The Integrated Quality and Governance team has worked with NHSP healthcare organisations to clarify the requirements for provider SI management SI reports are now sent to a dedicated NHSP in-box Timeliness for processing of reports has improved as required Clinical Quality forums cover provider SI management and review The back log of incomplete investigations has been completed and cleared Further detail of SIs reported to NHSP for each provider in 2010/11 is given in the following pages. NHSC/P SI Annual Report 10/11 Page 19 of 23 August 2011 Peterborough & Stamford Hospitals Foundation Trust The number of SIs reported by PSHFT in 2010-11 has increased. Work to improve reporting processes has been on-going with the hospital. PSHFT are seen by the SHA as low reporters of SIs in the East of England. Provider reporting and monitoring processes have been further developed to ensure that all incidents that meet the serious incident definition are reported appropriately as SIs to NHSP. Work to improve the timeliness of reporting and the completion of investigations will continue with the provider and the implementation of learning through investigations and reviews will be monitored through the clinical quality review process. Cambridgeshire & Peterborough NHS Foundation Trust There has been an increase in the number of reported suicides. The quality of risk assessments and care planning was highlighted as a theme in the NHSP review of final reports relating to suicide. CPFT have put actions in place as part of the suicide prevention work which should address these areas, but monitoring of this will need to continue. CPFT also plan to establish a joint Suicide Prevention Group linking with GPs to ensure appropriate risk assessment at all stages. Outcomes from this group will need to be reviewed quarterly to ensure it is fit for purpose. Peterborough Community Services There has been an increase in the number of SIs reported by PCS in 2010-11. Serious incidents have been under-reported within community services in previous years. The development of serious incident reporting processes within PCS, increased awareness of the serious incident definition and an improvement in the reporting culture has led to an increase of serious incident numbers. The development of reporting processes achieved by PCS in 2010/11 will continue to be monitored as services transfer to new providers in 2011/12. PCS are lower reporters of Pressure Ulcer (PU) SIs than CCS, there may of course be several reasons for this. It is essential that learning is collated to ensure that if treatment of vulnerable patients in PCS results in development of less PU’s that best practice is shared in a timely way across organisations. HMP Peterborough HMP Peterborough continue to engage with NHSP and the SI reporting processes, reporting healthcare SIs when they occur. One serious incident has been reported this year. NHS Peterborough The number of SIs reported by NHSP has increased this year. Work has been ongoing to improve awareness of SIs reporting by independent providers. There have been a number of multi-agency investigations that have led to shared learning across the health and social care economy and improvements to pathways of care. NHSC/P SI Annual Report 10/11 Page 20 of 23 August 2011 Appendix 6 – Examples of action taken by providers following SI investigation Training Retraining for ambulance clinicians in anaphylactic care. Introduction of formal human factors training for theatre staff, to compliment the use of the World Health Organisation safe surgery checklist. Documentation The VTE Risk Assessment Form amended to facilitate and prompt reassessment after 24 hours, including a consideration by specialities to ensure it is sensitive to particular requirements of the patient population. Joint development across primary and secondary care of clear, accessible information for families and carers of terminally ill patients that covers all end of life services. Clinical responsibility All allied health professionals informed regarding their responsibility to document in the patient records and inform the nurse in charge of any treatment regimes on ward patients. Reminder in the staff bulletin of the importance of maintaining a professional relationship with their patients at all times and to report any incidents at an early stage. Policy development Development of a standard operating procedure for communicating assessment outcomes. Review of the current evidence base and risk/benefits of prophylactic antibiotic use in specific care. Pathway management Establishment of a community project group to review the role of medical staff with the aim of embedding and collocating medical staff within their pathway team. Review of care pathway for mental health teams including identifying associated care records documentation required. NHSC/P SI Annual Report 10/11 Page 21 of 23 August 2011 Appendix 7 – Glossary Being Open Open communication of patient safety incidents that result in harm or the death of a patient while receiving healthcare. Carers Family, friends or those who care for the patient. The patient has consented to their being informed of their confidential information and to their involvement in any decisions about their care. Clinical Governance A framework through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish. Commissioning organisation An organisation with responsibility for buying services from service providers in either the public, private or voluntary sectors. Health economy All stakeholders that contribute to healthcare in a specified region. Incident An event or circumstance which could have resulted, or did result in unnecessary damage, loss or harm such as physical or mental injury to a patient, staff, visitors or members of the public. Independent contractors GPs, dentist, optometrists and community pharmacists that provide services as independent businesses contracted with the commissioner. Infection control Processes, policies and procedures used to minimize the risk of spreading infections, especially in healthcare facilities. Information Governance The structures, policies, procedures, processes and controls implemented to manage information in such a way that it supports the organisations regulatory, legal, risk, environmental and operational requirements. Never Events Patient safety incidents that should not occur if the available preventative measures have been implemented by healthcare provider. NHS-Funded Healthcare Healthcare that is partially or fully funded by the NHS, regardless of the location. NPSA National Patient Safety Agency. An organisation that leads and contributes to improved, safe patient care by informing, supporting and influencing the health sector. Patient pathway The care and treatment received by the patient as seen from the patient’s perspective rather than that given by individual health care organisations Provider organisations Organisations that NHSC and NHSP commission to provide healthcare to its population. These organisations provide a wide range of healthcare including acute, primary medical and dental, ambulance, community and mental health services NHSC/P SI Annual Report 10/11 Page 22 of 23 August 2011 Root cause A cause which leads to an outcome or effect of interest. Commonly, root cause is used to describe the depth in the causal chain where an intervention could reasonably be implemented to change performance and prevent an undesirable outcome. Safeguarding children and vulnerable adults Ensuring that people live free from harm, abuse and neglect and, in doing so, protecting their health, wellbeing and human rights. Children, and adults in vulnerable situations, need to be safeguarded. For children, safeguarding work focuses more on care and development; for adults, on empowerment, independence and choice. Severe Harm A patient safety incident that appears to have resulted in permanent harm to one or more persons receiving care. SI Serious Incident - An incident that meets the definition set out by the NPSA: A serious incident requiring investigation is defined as an incident that occurred in relation to NHS-funded services and care resulting in: Unexpected or avoidable death of one or more patients, staff, visitors or members of the public; Serious harm to one or more patients, staff, visitors or members of the public or where the outcome requires lifesaving intervention, major surgical/medical intervention, permanent harm or will shorten life expectancy, or result in prolonged pain or psychological harm (this includes incidents graded under the NPSA definition of severe harm); A scenario that prevents or threatens to prevent a provider organisation’s ability to continue to deliver health care services, for example, actual or potential loss of personal/ organisational information, damage to property, reputation or the environment, or IT failure; Allegations of abuse; Adverse media coverage or public concern for the organisation or the wider NHS; One of the core set of ‘Never Events’ as updated on an annual basis Strategic Health Strategic health authorities (SHA) manage the local NHS on Authority behalf of the secretary of state. Their responsibilities include making sure local health services are of a high quality and are performing well. The local SHA, EoE NHS, covers the east of England. Thematic review A review of related incidents to determine if there are common root causes that should be addressed to prevent re-occurrence of similar incidents. Unexpected Death Where natural causes are not suspected. Local organisations should investigate these to determine if the incident contributed to the unexpected death NHSC/P SI Annual Report 10/11 Page 23 of 23 August 2011