PMD 10. Reprod.physiol - campus
advertisement

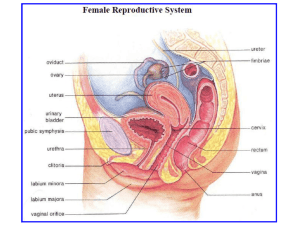
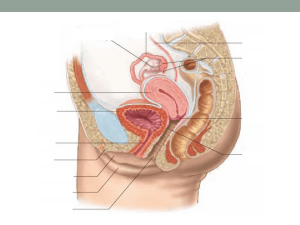
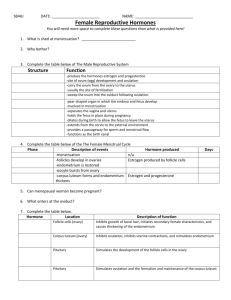
D’YOUVILLE COLLEGE PMD 604 - ANATOMY, PHYSIOLOGY, PATHOLOGY II Lecture 10: Male & Female Reproductive Systems G & H chapters 80 & 81 1. Anatomy of Male Reproductive Tract (fig. 80 - 1 & ppt. 1): • testes: primary sex organs suspended via spermatic cord in scrotum; blood supply: testicular artery surrounded by venous network (pampaniform plexus) facilitates temperature regulation - lobules contain seminiferous tubules (site of spermatogenesis) (fig. 80 – 2 & ppt. 2) - endocrine interstitial cells of Leydig (source of androgens) (figs. 80 - 7, 80 - 8 & ppts. 3 & 4) - epididymis: secretes seminal fluid (about 10% of semen) connects testis with vas deferens (sperm duct); approx. 6 meters of coiled tubules in epididymis - vas passes into body within spermatic cord & loops medially over ureter to descend posterior wall of urinary bladder; surgical interruption = 'vasectomy' • accessories: seminal vesicles empty into proximal parts of vasa deferentia; secrete seminal fluid (approximately 60% of volume of semen) - prostate gland: receives urethra from urinary bladder and is site of junction of vasa deferentia with urethra (combined reproductive and urinary passageway from this point to exterior); secretes prostatic fluid (about 30% of semen) - bulbourethral glands: join urethra near bulb of penis; secrete mucus - urethra extends from urinary bladder through prostate (prostatic part), pierces urogenital diaphragm (membranous part), and passes out penis to exterior (spongy part); combined reproductive and urinary passageway • penis (fig. 80 - 6 & ppt. 5): copulatory organ composed of three masses of erectile tissue: - corpus spongiosum: features proximal swelling (bulb) and distal swelling (glans); conveys urethra to exterior; glans may be covered by prepuce (foreskin) - corpora cavernosa: dorsal masses; diverge proximally (crura of penis) 2. Physiology of Male Reproduction: • spermatogenesis (fig. 80 - 2 & ppt. 6): - spermatogonia (diploid sperm mother cells) at periphery of seminiferous tubule ---> primary spermatocytes (diploid cells that enter meiosis I) ---> secondary spermatocytes (haploid cells that enter meiosis II) (fig. 80 - 3 & ppt. 7) ---> spermatids (haploid cells that mature into spermatozoa (fig. 80 - 4 & ppt. 8); maturation = spermiogenesis) - latter processes occur in intimate association with nutritive sustentacular (Sertoli) cells PMD 604, lec 10 - p. 2 - - spermatozoa: headpiece includes condensed male pronucleus (haploid set of chromosomes, including either X or Y) - acrosome (specialized lysosome) aids penetration of egg membranes during fertilization - tail is composed of a flagellum (with typical core of microtubules); proximal part also contains mitochondria that provide energy (ATP) to support tail motility • hormonal relationships (fig. 80 - 10 & ppt. 9): - gonadotropin releasing hormones: (from hypothalamus) regulate pituitary gonadotropins: - follicle stimulating hormone (FSH): stimulates spermiogenesis in testis; collaborates with testosterone to promote spermatogenesis - luteinizing hormone (LH): supports testosterone secretion by interstitial cells - human chorionic gonadotropin (hCG): (from placenta) stimulates testosterone secretion in genital ridge & embryonic testes in fetus; Y chromosome contains sex-determining region (SRY) that codes for SRY protein - SRY protein promotes male developmental pattern - testosterone: promotes development of primary reproductive structures (acts in fetus, neonate & resumes in adolescents & adults) (fig. 80 - 9 & ppt. 10) - promotes growth & proliferation of spermatogonia, development of secondary sex characteristics (e.g., distribution of body hair, including baldness based on genetics, muscular hypertrophy, enlargement of larynx) - inhibin: (from Sertoli cells) imposes negative feedback inhibition of hypothalamic-hypophysial-gonadal axis (especially FSH) to control rate of spermatogenesis • erection and orgasm: penis (normally flaccid, inferiorly directed) becomes rigid and erect during sexual excitation (evoked by sensory stimuli from external genitalia as well as psychic stimuli) - parasympathetic nerve activity causes hyperemia of erectile tissues producing an erection (renders penis suitable for intromission and deposit of semen in female reproductive tract); PNS nerve endings may release or trigger secretion of NO (vasodilator) - sympathetic nerve signals cause emission & ejaculation (sexual climax) 3. Anatomy of Female Reproductive Tract (figs. 81 - 1, 81 - 2 & ppts. 11 & 12): • ovaries (fig. 81 - 4 & ppt. 13): primary sex organs in pelvis; produce ova; secrete sex hormones - primordial follicles (primary oocyte + granulosa cells) are formed at birth from germinal epithelium (oogonia) - granulosa cells nourish ovum & produce estrogens & progesterone - primary follicles: growth of ovum & development of additional layers of follicle cells (granulosa cells & thecal cells) - vesicular follicles: follicles secrete fluid into developing cavity (antrum); also secrete estrogens, which increase sensitivity to gonadotropins & accelerate growth of follicles PMD 604, lec 10 - p. 3 - - mature follicle: only one (of perhaps a dozen follicles that commenced the cycle) will 'ripen' to be ready for ovulation; bulges at surface of ovary (stigma) & erosion of surface follicle cells permits bursting & release of ovum with associated granulosa cells (corona radiata); triggered by LH surge (figs. 81 - 3, 81 - 5 & ppts. 14 & 15) - corpus luteum: follicle cells remaining in ovary following ovulation, undergo luteinization, a process that includes lipid accumulation & synthesis of larger amounts of progesterone PMD 604, lec 10 - p. 4 - • uterus (fig. 81 - 1, 81 - 2 & ppts. 11 & 12): - composed of body, fundus & cervix; wall is comprised of perimetrium, myometrium & endometrium - endometrium passes through cycles of buildup (proliferative phase), secretion (secretory phase) & deterioration with sloughing of necrotic material (menstrual phase) (fig. 81 - 8 & ppt. 16) - uterine tubes: terminate near ovaries with fimbriae at ends & ciliated lining • vagina (birth canal): inferior to uterus, lined with stratified squamous mucosa • vulva: labia majora and labia minora enclose vestibule containing clitoris (homologue of penis), opening of urethra and vaginal orifice (fig. 81 - 1 & ppt. 11) 4. Mammary Glands: • modified sweat glands serving to produce milk to nourish newborn - glandular units (alveoli) empty into lactiferous ducts that communicate with openings in the external nipple (surrounded by areola); development stimulated by estrogens, but final maturation & function depends on progesterone & prolactin 5. Physiology of Female Reproduction: • hormonal relationships (figs. 81 - 10 & ppt. 17): - hypothalamus hormones: gonadotropin releasing hormones that regulate pituitary gonadotropins - anterior pituitary hormones: follicle stimulating hormone (FSH): for follicle growth in ovary - luteinizing hormone (LH): for follicle maturation, estrogen secretion & progesterone secretion (fig. 81 - 7 & ppt. 18) - LH surge (near mid cycle) causes ovulation; LH stimulates follicular residue to form corpus luteum, which secretes progesterone and some estrogens; LH maintains corpus luteum - ovarian hormones (figs. 81 - 6, 81 - 7 & ppts. 18 & 19): prior to ovulation (follicular phase), ovary secretes mainly estrogen with some progesterone just before ovulation; after ovulation (luteal phase), ovary secretes predominantly progesterone (fig. 81 - 3 & ppt. 14) - estrogens: proliferation of mammary glands and glands of endometrium; enlargement of pelvic dimensions, development of secondary sex characteristics (female distribution of body fat, rapid but shortened growth in early puberty, development of pubic and axillary hair) - progesterone: promotes secretion by mammary gland & by endometrium • ovarian cycle (ppt. 21): - follicular phase (preovulatory phase): (approx. first 14 days) follicles enlarge, become vesicular with primary oocyte completing first meiosis; mature follicle (ready for ovulation); mostly directed by FSH from anterior pituitary with help of LH PMD 604, lec 10 - p. 5 - - luteal phase (post ovulatory phase): LH surge triggers ovulation and development of corpus luteum; progesterone level rises and produces a strengthening of estrogen's negative feedback on anterior pituitary inhibiting further output of gonadotropins; inhibin, also produced by granulosa cells exerts feedback inhibition (especially of FSH) PMD 604, lec 10 - p. 6 - • uterine cycle (fig. 81 - 8 & ppts. 16 & 21): - proliferative phase: estrogens promote thickening of endometrium (rich blood supply, extensive glandular development) - secretory phase: progesterone from corpus luteum promotes glandular secretion, preparation of endometrium for implantation - menstrual phase: in absence of implantation, negative feedback on anterior pituitary causes deterioration of ovarian corpus luteum and resulting decline in progesterone leads to sloughing off of endometrium constituting the menstrual discharge (4 - 5 days) • regulation of non-pregnant reproductive cycle: (ppts. 20 & 21) - following menses, pituitary FSH and LH rise, initiating next follicular phase of ovary - estrogens from maturing follicles promote proliferative phase of uterine endometrium • rising estrogen levels cause positive feedback upon anterior pituitary causing gonadotropin surges (especially LH); ovulation ensues • corpus luteum formation in ovary marks beginning of luteal phase with progesterone dominating hormonal picture • progesterone promotes secretory phase of uterine endometrium and potentiates estrogen's negative feedback inhibition of AP gonadotropins • corpus luteum regresses (lack of LH support); endometrium deteriorates with lack of progesterone support; menses begins