Future Directions for a Māori Dental Therapy

FUTURE DIRECTIONS FO R A MĀORI DENTAL
THERAPY WORKFORCE
FIONA CRAM, JUDY OAKDEN AND NAN WEHIPEIHANA
Published in March 2011 by the
Ministry of Health
PO Box 5013, Wellington 6145, New Zealand
ISBN 978-0-478-37433-9 (online)
HP 5292
This document is available on the Ministry of Health
’s website: http://www.moh.govt.nz
The Team
In 2008 the Ministry of Health funded Research Evaluation Consultancy Ltd to undertake an analysis of future directions for a Māori Dental Therapy workforce. The research was undertaken by Fiona Cram, Judy Oakden and Nan Wehipeihana (with the assistance of
Kataraina Pipi, Kellie Spee and Laurie Porima).
Acknowledgements
The Ministry of Health has walked alongside us in the development of this research report, providing us with insigh ts into the field of Māori oral health and feedback on drafts. Kia ora ki a
Peter Himona, Charrissa Makowharemahihi, Monique Priston, Robin Whyman, Paula Searle and Teresa Wall. Peter ’s assistance with data has also been invaluable.
Many thanks to the key informants who provided guidance and additional information during the development of this research report (see Appendix A). This has both grounded and broadened our perspective.
Thanks also to Dr Murray Thomson for additional dental therapist workforce data.
Future Directions for a Māori Dental Therapy Workforce
iii
Abbreviations
APC
AUT
DCNZ
DHB annual practising certificate
Auckland University of Technology
Dental Council of New Zealand
District Health Board
DHBNZ
DTTAG
District Health Boards of New Zealand
Dental Therapy Technical Advisory Group
HPCA Act 2003 Health Practitioners Competency Assurance Act 2003
HWAC Health Workforce Advisory Committee (disestablished September 2006)
NCEA
Otago
SDS
TEC
National Certificate of Educational Achievement
University of Otago
School Dental Service
Tertiary Education Commission
Glossary
mihi whakatau speech of greeting oranga niho oral health tamariki rangatahi
Māori children
Māori young people
Te Ao Marama New Zealand Māori Dental Association
iv
Future Directions for a Māori Dental Therapy Workforce
Table of Contents
ABBREVIATIONS
EXECUTIVE SUMMARY
1.
INTRODUCTION
2.
POPULATION PROJECTIONS
3.
MĀORI ORAL HEALTH SERVICE REQUIREMENTS
3.1
Māori oral health status
3.2
Normative needs
3.3
Consumer awareness – expectation
3.4
Demand for oral health services
3.5
Use of oral health services
3.6
Oral health service requirements
4.
THE SUPPLY OF MĀORI DENTAL THERAPISTS
4.1
2006 Māori dental therapy workforce
4.2
2018 Māori dental therapy workforce
4.3
Assumptions
4.4
Summary
5.
MĀORI AND SECONDARY SCHOOL SCIENCE
5.1
Māori student participation in science
5.2
Māori student attainment in science
5.3
Ensuring success in science
5.4
Summary
6 TERTIARY EDUCATION IN DENTAL THERAPY
6.1
Recruiting Māori students
6.2
Retaining Māori students
6.3
Summary
7 DENTAL THERAPY WORK ENVIRONMENT
7.1
Transition to work
7.2
Working environment
7.3
Summary
8 OVERALL SUMMARY AND RECOMMENDATIONS
8.1
Four future scenarios
8.2
Policy implications
REFERENCES
IV
VII
24
24
24
26
18
18
21
22
12
12
14
16
17
27
27
27
30
3
3
5
5
6
6
7
8
8
9
10
11
1
2
Future Directions for a Māori Dental Therapy Workforce
v
APPENDICES
Appendix A: Method
Appendix B: Supply of dental therapists
Appendix C: Including productivity in the Māori workforce supply calculations
ENDNOTES
LIST OF TABLES
Table A: Future scenarios for the dental therapy workforce, 2018
Table 1: Population projections (number and percent of total age group population) for
0 –17 year olds, by ethnicity
Table 2: Participation of Māori and non-Māori student cohort in science, Years 11–12,
2007 –2009
Table 3: Attainment of Māori and non-Māori student cohort in science, Years 11–13,
2007 –2009
Table 4: Recruitment of Māori students into the AUT Bachelor in Health Science in
Oral Health programme
Table 5: Recruitment of Māori students into the Otago Bachelor of Oral Health programme 1
Table 6: Future scenarios for the dental therapy workforce, 2018
Table 7: Estimated gain (+) and loss ( –) of dental therapists from the workforce,
2006 –2018
Table 8: Productivity, caseload and the number of Māori dental therapists required in
2006, and projected workforce requirements for 2018: Scenario 1 x
2
14
15
20
21
28
35
36
32
34
36
38
LIST OF FIGURES
Figure 1: Severity of dental caries (dmf/DMF) by fluoridated and non-fluoridated for 5year-olds, SDS data 2003 –2009 and data projections for 2013 and 2018
Figure 2: Severity of dental caries (dmf/DMF) by fluoridated and non-fluoridated for
Year 8 children, SDS data 2003 –2009 and data projections for 2013 and
2018
Figure 3: Percentage of nonMāori and Māori dental therapy workforce by age group
Figure 4: Māori and non-Māori participation rate (percentage) in Year 11–13 NCEA science subjects, 2004 –2007, and predicted participation in 2013 and 2018
Figure 5: Māori and non-Māori attainment (percentage) in Year 11–13 NCEA science subjects, 2004 –2007, and predicted attainment in 2013 and 2018
Figure 6: Age-standardised participation rates in tertiary education per 100 population aged 15 years and over by ethnic group, 1994 –2008
LIST OF DIAGRAMS
Diagram 1: Model of oral health service requirements
Diagram 2: Māori health and disability workforce development pathway
4
4
8
13
15
19
vi
Future Directions for a Māori Dental Therapy Workforce
Executive summary
The aim of the present project was t o collate information on the status of the Māori dental therapy workforce, and analyse the needs of the Māori dental therapist workforce over the next eight years.
The present paper examines the current and future needs of the Māori dental therapy workforce in terms of the oral health service requirements of Māori and the supply of Māori dental therapists. These were considered within the context of a Māori 0–17-year-old population which is projected to grow by 13.7 percent to just under 300,000 by 2018 (or 21.2% of the young people in this age group). If nothing else changes, this growth in population alone can be expected to place heavier demands on dental therapy services in the next eight years.
The premise underlying the analysis of the supply of Māori dental therapists is that every Māori child and young person (aged 0 –17 years) should receive optimal oral health services. Four scenarios were explored for the provision of these services.
1. Growth in the oral therapy workforce that aligns with what the current institutions can supply.
2. Every Māori child receiving optimal oral health care, with a growing Māori workforce contributing to this service provision.
3. The proportion of Māori in the oral health therapy workforce aligning with the proportion of the population under 18 years of age that is Māori.
4. Every Māori child being able to receive optimal oral health care from a Māori dental therapist if they or their whānau choose.
Māori oral health service requirements
The components of a model of oral health service requirements that have been explored for Māori 0–17-year-olds are shown on the right.
Looking at oral health status, Māori fiveyearolds and Māori in Year 8 (12-yearolds) had a higher severity of dental caries than their nonMāori/non-Pacific peers in
2002 through 2009. Those children in fluoridated areas had better oral health status than those in non-fluoridated areas. The oral health status of Māori children is predicted to improve over the next eight years although the disparity will remain.
Normative need is expert-defined standards for oral health status – for Māori children and young people, the same as the oral health status of their nonMāori/non-Pacific peers living in fluoridated areas. This standard is expected to change over the next eight years in line with the predicted improvement in the oral health status of non-Maori children and young people living in non-fluoridated regions.
Māori consumer awareness and expectations of the oral health of 0 –17-year-olds should increase over the next eight years given the emphasis on oral health promotion and the priority being given to Māori oral health.
Demand for oral health services is shaped by oral health status and normative needs, along with consumer awareness and expectations. Raising Māori awareness and expectations will undoubtedly increase demand for oral health services.
Future Directions for a Māori Dental Therapy Workforce
vii
Use of oral health services depends on demand and also on service acceptability to Māori.
When an acceptable service is offered Māori use increases, and acceptable oral health services influence awareness and expectations as well as contribute to improved oral health status.
Oral health service requirements are driven by Māori awareness and expectations and the provision of accessible services. The Māori dental therapy workforce has an important role to play in the provision of accessible oral health services for this age group. However, the demands on this workforce will be great if the oral health disparities experienced by this growing population of Māori 0–17-year-olds remains only slightly improved. Urgent attention is therefore required to increase the capacity of the dental therapy workforce so that it can contribute to improving the oral health of Māori children and young people.
Supply of Māori dental therapists
In 2006, 65 (10%) of the 650 dental therapists holding an Annual Practising Certificate (APC) were M āori. This is well below the 130 Māori dental therapists that would have been needed for the proportion of Māori dental therapists in the workforce to be aligned with the proportion of
Māori 0–17-year-olds in the 2006 population. This number increases to 153 Māori dental therapists when the ratio is adjusted to 59.6 Māori dental therapists per 100,000 Māori
0 –17-year-olds. When productivity is taken into account there is a further increase to between
178 and 222 Māori dental therapists that would have been needed in 2006 to provide optimal oral health care to Māori 0–17-year-olds.
The 2018 projection for the dental therapy workforce is 788 dental therapists, including 52 Māori dental therapists remaining in the workforce from 2006. Aligning the proporti on of Māori in the workforce with projections about the proportion of Māori 0–17-year-olds in 2018 would require a total of 169 Māori dental therapists. When productivity is taken into account, between 174 and
208 Māori dental therapists will be needed in 2018 to provide optimal oral health care to Māori
0 –17-year-olds.
It is acknowledged that some Māori 0–17-year-olds will see non-Māori dental therapists and other oral health professionals, and that some Māori dental therapists may work with all whānau members, may work with nonMāori, and/or may only practise dental hygiene (rather than therapy). The projections for the general dental therapy workforce also suggest that it will have the potential to deliver optimal oral health care to Māori children and young people if dental therapists are culturally competent.
Educational pathways to dental therapy
The pathway for Maori into tertiary education in dental therapy begins with people ’s experiences prior to secondary school. This includes role models, academic preparation, and the promotion of dental therapy as a career option. This promotion needs to include the provision of good oral health care. Secondary school education (including the attainment of secondary school science, particularly biology) or second chance entry provide pathways into a tertiary education institute, namely the University of Otago or AUT University (see diagram above).
viii
Future Directions for a Māori Dental Therapy Workforce
Secondary
At secondary school twothirds of Māori participate in science at Year 11 but this participation drops to around 22 percent in Year 13. The low attainment of Māori students in science at
Year 11 undoubtedly contributes to this drop-off in participation in later years. Of the Māori students participating in Year 11 science in 2007, 6.8 percent attained Year 13 science in 2009
(compared to 21.4% for nonMāori students).
Māori student participation in science is predicted to increase in Years 11 and 12 over the next eight years, but decrease in Year 13. Māori student attainment in science in all years is predicted to increase over the next eight years; however, by 2018 the number of Māori students attaining Year 13 science is predicted to still be less than 1000.
More Māori students need to be encouraged to participate in science at secondary school. The attainment of Māori students in science also needs to be addressed as a matter of urgency so that at least one in five students who participate in Year 11 science subsequently passes
Year 13 science. Investment in the professional development of teachers, the provision of role models and mentors, and possibly the revision of the science curriculum, will assist the participation and attainment of Māori students.
Tertiary
The University of Otago (Otago) and Auckland University of Technology (AUT) each offer a bachelors degree that is now the minimum requirement for anyone entering the dental therapy workforce. Students graduate with a dual qualification in dental therapy and dental hygiene.
The recruitment of Māori into dental therapy programmes remains an issue, with very few Māori students entering the programmes at AUT and Otago over the past four years.
Foundation courses at each institution provide a pathway into dental therapy for mature (secondchance) students. Both institutions also offer supp ort for Māori students, and there are scholarship programmes available that can help alleviate financial pressures.
Dental therapy working environment
Since 2004 dental therapists have been able to be employed outside the public service. While it is anticipated that new dual-qualified graduates will find private practice attractive, it is too early to say what impact this will have on the dental therapy workforce.
The transition of new graduates into the workforce can be facilitated by mentoring, career counselling and professional networks such as that offered by
Te Ao Marama (the New Zealand Māori Dental Association).
Improvements in pay and working conditions for all dental therapists may help retain them in the public service. This may also make dental therapy a more attractive career option and assist in the recruitment of Māori students into the tertiary programmes.
Māori preferred-employer criteria define a working environment for Māori dental therapists that supports them to be Māori. These criteria include support for Māori staff professional development (including cultural development) and the provision of health services that recognise whānau and community contexts. These factors facilitate the recruitment and retention of Māori staff into a workplace.
Future Directions for a Māori Dental Therapy Workforce
ix
Summary
The analysis related to each of the four scenarios is summarised in Table A. The most likely solution to Māori oral health needs in 2018 is the provision of accessible oral health services by a combined Māori and non-Māori dental therapy workforce. This should not detract from the goal of building the Māori dental therapy workforce so that it is at least reflective of the proportion of Māori in the 0–17-year-old age group.
Table A: Future scenarios for the dental therapy workforce, 2018
Scenario Workforce requirement(s)
1. Growth in the oral therapy workforce that aligns with what the current institutions can supply
The estimated dental therapy workforce in 2018, based on projected losses due to workforce retirements and gains from graduates entering the workforce, is 788 dental therapists.
Based on 2006 percentages, approximately 10 percent of these dental therapists will be Māori (i.e. 79). If this includes 52 from the 2006 workforce, then the institutions need to graduate between 2 and 3 Māori students each year from 2007 to 2017. This is in line with current institutional data.
2.
Every Māori child receiving optimal oral health care, with a growing Māori workforce contributing to this service provision
3.
The proportion of Māori in the oral health therapy workforce aligning with the proportion of the
0
–17-year-old population that is Māori
4. Every Māori child being able to receive optimal oral health care from a
Māori dental therapist if they or their whānau choose
Applying the 2006 ratio of 59.6 dental therapists per 100,000 population indicates that, in 2018, 465 of the projected workforce of 788 dental therapists (see Scenario 1) will be needed to supply oral health care to the nonMāori 0–17-year-old population.
Committing the remaining 323 dental therapists to the provision of oral health servic es to Māori will give a ratio of 110.8 dental therapists per
100,000 Māori 0–17-year-olds. This ratio can potentially supply optimal oral health care to Māori 0–17-year-olds.
The projected 0
–17-year-old Māori population in 2018 is 291,840, or
21.5 percent of the total projected population in this age group.
Based on the general dental therapy workforce projection in Scenario 1,
167 of the 788 dental therapists in 2018 will be Māori if the workforce aligns with the population.
It is predicted that 52 of the 2006 Māori dental therapy workforce will still be working in 2018.
Therefore 115 new Māori dental therapists will be needed
– that is, just over 10 Māori graduates each year from 2007 to 2017.
For the optimal oral health care for Māori 0–17-year-olds to be provided by Māori dental therapists in 2018 between 10 and 13 new Māori dental therapists would need to enter the workforce each year from 2007 to
2018.
x
Future Directions for a Māori Dental Therapy Workforce
Policy implications
The following policy implications arise from the present analysi s of the Māori dental therapy workforce.
1. Māori children and young people urgently need good oral health care. DHBs need to hold all oral health providers, including themselves , accountable for the oral health of Māori children and young people. This may mean, for example, cultural competency training for nonMāori oral health professionals, the purchasing of more Māori oral health services, and the provision of oral health services at times and in places that are most accessible for Māori whānau.
2. Māori secondary school student science attainment needs to increase so that at least
20 percent of those participating in Year 11 science attain Year 13 science. While general support, monitoring and individualised pathways for Māori secondary school students may gain some traction, investment in the professional development of teachers
(Te Kotahitanga) is also showing promise. In addition the science curriculum itself may need to be made more relevant to Māori students and their whānau, offer students more individual choice, be made more interesting and take a more cross-disciplinary approach.
3. The number of Māori training to be dental therapists needs to increase. Both the
University of Otago and AUT need to actively recruit Māori students into their programmes. Each programme needs to commit to enrolling at least 8 –10 Māori dental therapy students each year for the next six years if the 2018 dental therapy workforce is going to have a representative number of Māori dental therapists – that is, a Māori dental therapy workforce that is proportionate to the 0 –17-year-old Māori population in 2018.
This recruitment should be actively supported by scholarships for these students.
4. The provision of other tertiary options for educating Māori dental therapists should be explored, including the funding of a programme developed by a wānanga and/or the provision of scholarships so that Māori students can train in Australian programmes.
5. DHBs need to make the working conditions and remuneration of dental therapists in the public service more attractive. For Māori dental therapists this also means making the workplace supportive of them being Māori and practicing dental therapy in a way that is compatible with this.
Future Directions for a Māori Dental Therapy Workforce
xi
1. Introduction
The vision of the Ministry of Health ’s Māori health workforce development plan, Raranga
Tupuake, is ‘... to build a competent, capable, skilled and experienced Māori health and disability workforce over the next 10 –15 years’ . Three goals to achieving this vision are described in
Raranga Tupuake (Ministry of Health 2006b, p.2):
1. Increase the number of Māori in the health and disability workforce,
2. Expand the skill base of the Māori health and disability workforce, and
3. Enable equitable access for Māori to training opportunities.
Dental therapists provide oral health care to children and young people up to 17 years of age, and can provide oral health care for adults if they undertake the necessary (adult scope) training.
Māori are under-represented in the dental therapy workforce (DHBNZ, 2004). The present project examined the current and future needs of the Māori dental therapy workforce. The aim was:
To collate information on the status of the Māori dental therapy workforce, and analyse the needs of the Māori dental therapist workforce over the next eight years.
The premise underlying the analysis of the supply of Māori dental therapists is that every Māori child and young person (aged 0 –17 years) should receive optimal oral health services. Four scenarios were explored for the provision of these services.
1. Growth in the oral therapy workforce that aligns with what the current institutions can supply.
2. Every Māori child receiving optimal oral health care, with a growing Māori workforce contributing to this service provision.
3. The proportion of Māori in the oral health therapy workforce aligning with the proportion of
Māori in the population under 18 years.
4. Every Māori child being able to receive optimal oral health care from a Māori dental therapist if they or their w hānau choose.
This project links the current and future needs of the Māori dental therapy workforce to:
Māori oral health service requirements
the supply of M āori dental therapists.
Māori oral health service requirements are related to:
Māori oral health status consumer awareness and expectations
demand for, and use of, oral health services.
The supply of Māori dental therapists is, in turn, linked to:
Māori secondary school science achievement
dental therapy education
the dental therapy work environment.
Each of these service and supply areas is explored following an initial overview of population projections for the 0 –17 age group. Information related to each of the four scenarios has been highlighted in the body of the report.
The report concludes with summary comments, a discussion of each scenario, and policy implications.
Future Directions for a Māori Dental Therapy Workforce
1
2. Population projections
In 2006 there were 1,081,220 0 –17-year-olds, with this age group making up just over a quarter
(25.8%) of the national population.
1 The population projections for 0 –17-year-olds include the growth of the Māori population in this age group and the shrinkage of the ‘European and Other
(including New Zealanders) ’ population (see Table 1). By 2013 it is projected that there will be
277,200 Māori under the age of 18 years. This figure is projected to increase to just under
300,000 by 2018 (N = 291,840). This is an increase of 13.7 percent from 2006 to 2018. The
0 –17-year-old Māori population is then projected to surpass the 300,000 mark by 2023. At each of these projected dates the proportion of the 0 –17-year-old population that is Maori increases, from 20.1 percent in 2006 to 21.5 percent in 2023.
Table 1: Population projections (number and percent of total age group population) for 0
–17 year olds, by ethnicity
Year
2006
2013
2018
2023
European/Other
N
783,200
766,960
756,420
750,570
%
61.4
57.7
55.0
52.6
Māori
N
256,720
277,200
291,840
306,570
%
20.1
20.9
21.2
21.5
Pacific
N
130,530
154,270
170,840
187,470
Source Statistics New Zealand 2006 Census Data and Projections
%
10.2
11.6
12.4
13.1
Asian
N
104,470
130,090
156,390
183,770
%
8.2
9.8
11.4
12.9
Scenario 3. Workforce aligned with the population
In 2006, 65 of the 650 dental therapists holding Annual Practising Certificates (APCs) were Māori. If Māori are represented in the dental therapy workforce proportionately to the Māori population under 18 years, then at least 20 percent of this workforce should currently be Māori – that is, 130 dental therapists.
Over the next eight years the proportion of Māori in the dental therapy workforce should grow to at least 21.2 percent. In 2018 the number of dental therapists is predicted to be
788 (see Appendix B). In order for this workforce to be proportionate to the Māori population under 18 years, 167 of these dental therapists wi ll need to be Māori.
2
Future Directions for a Māori Dental Therapy Workforce
3. Māori oral health service requirements
This section examines Māori oral health service requirements using the Australian dental labour force model (AIHW Dental Statistics and Research Unit, 1998; Australian Health Minister ’s
Advisory Council, 2001). See Diagram 1 for a simple representation of this model. This model links oral health service requirements to:
normative needs driven by the oral health status of the population
use of services driven by demand and consumer awareness/expectation.
T he components of this model are examined below, beginning with Māori oral health status.
Diagram 1: Model of oral health service requirements
Source AIHW Dental Statistics and Research Unit (1998)
3.1 Māori oral health status
Currently the most reliable source of data on the oral health of children and young people is the
School Dental Service (SDS). Koopu & Keefe-Ormsby (2007) note that there are quality issues with the SDS data.
1. Ethnicity has only been recorded since 2002, and even then the ethnicity classification is likely to undercount M āori.
2. The use of dmf/DMF (decayed, missing or filled teeth) as a measure of dental disease does not include gum disease or the reasons teeth are missing.
The 2003 –2009 SDS data on the oral health of 5-year-olds and Year 8 (12-year-old) children highlig hts the oral health disparities between Māori and non-Māori/non-Pacific (‘Other’) children.
Māori children in both age groups, regardless of fluoridation status, had a higher severity of dental caries (dmf/DMF) than ‘Other’ children.
2
The SDS data 3 has been used to predict the severity of dental caries (dmf/DMF) for 5-year-olds
(Figure 1) and year 8 children (Figure 2) in 2013 and 2018. The predictions for 2013 and 2018 for 5-year-olds are for a decrease in the severity of dental caries in Māori children living in nonfluoridated and fluoridated areas. The severity of dental caries in Other children living in fluoridated areas is not predicted to change, whereas there is a sharp decline predicted in Other children living in non-fluoridated areas so that in 2018 they are predicted to have the lowest severity of dental caries.
Predicted decreases in the severity of dental caries for Year 8 children are moderate for all children, with the gap between Māori and Other children maintained in 2013 and 2018 predictions.
Future Directions for a Māori Dental Therapy Workforce
3
Figure 1: Severity of dental caries (dmf/DMF) by fluoridated and nonfluoridated for 5-year-olds, SDS data 2003 –2009 and data projections for 2013 and 2018
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
ā ā
0.0
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
Year
Source SDS data from the Ministry of Health
20
12
20
13
20
14
20
15
20
16
20
17
20
18
Figure 2: Severity of dental caries (dmf/DMF) by fluoridated and nonfluoridated for Year 8 children, SDS data 2003 –2009 and data projections for 2013 and 2018
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
Year
20
12
20
13
20
14
20
15
20
16
20
17
20
18
Source SDS data from the Ministry of Health ā ā
4
Future Directions for a Māori Dental Therapy Workforce
3.2 Normative needs
Normative needs are defined by experts using agreed-upon standards (Orr, 1992). Need is defined if a group does not reach the desirable standard. For Māori children and young people a desirable oral health standard is the same oral health status as ‘Other’ children living with fluoridated water. This is expressed in Action Area 2 of the New Zealand Strategic Vision for
Good Oral Health: ‘Reduce inequalities in oral health outcomes and access to oral health services ’ (Ministry of Health, 2006a, p.13).
While the oral health status of Māori children and young people is predicted to improve in the next eight years (assuming the current level of service), the disparity between the oral health status of Māori and non-Māori children and young people is predicted to remain. Māori children and young people might therefore be expected to place a heavier demand on oral health services than presently because the normative need is shifting to a better standard of oral health. A commitment to the reduction of oral health disparities and the delivery of oral health care that matches the normative needs of Māori children and young people will require greater systemic responsiveness.
3.3 Consumer awareness – expectation
In addition to normative needs, Māori will have subjective (or psychosocial) perceptions that drive their demand for oral health services. If successful the promotion of oral health to Māori (a priority in Action Area 3 of the New Zealand oral health vision (Ministry of Health, 2006a)) will raise Māori awareness and expectations about the benefits of preventative oral health for children and young people. This greater awareness should, in turn, increase the demand for oral health care for this age group (cf. Australian Health Minister ’s Advisory Council, 2001).
The popular media also plays a role in the promotion of oral health. In the United States, reality television series such as Extreme makeover have resulted in increased demand for toothwhitening and veneers (Theobald, Wong, Quick & Thomson, 2006). It is not known what impact such programmes have on the oral health expectations of Māori.
Scenario 2. Optimal oral health care
In its modelling of future scenarios for the dental therapy workforce, the Health Workforce
Information Programme (2009) used three visit rates per day: 10.9, 12 and 15 (see
Appendix B). Māori oral health providers reported that a more realistic visit rate per day to meet current Māori need was 8.8 (see Appendix C). If equitable oral health services for
Māori children and young people are prioritised by non-Māori providers, it is anticipated that their productivity (i.e. visit rates per day) may drop, with a consequent need for more dental therapists.
If increasing Māori awareness and expectations increases demand for preventative oral health services, there will be a further reduction in the productivity of the dental therapists providing services to Māori children and young people.
Future Directions for a Māori Dental Therapy Workforce
5
3.4 Demand for oral health services
Demand for oral health services is shaped by oral health status and normative needs, along with consumer awareness and expectations (AIHW Dental Statistics and Research Unit, 1998).
If a concerted effort is made to provide oral health services and promotion for Māori children and young people, it is anticipated that their normative need will decline (i.e. the disparity will be reduced), but possibly not their demand for oral health services. The Australians have noted that the links between these components (normative need and consumer awareness and expectations) and demand for oral health services are seemingly counterintuitive in two key ways. First, high socioeconomic groups have better oral health status but use oral health services more than low socioeconomic groups; and second, improved child oral health status is accompanied by a higher proportion of the population visiting oral health providers (AIHW Dental
Statistics and Research Unit, 1998). Improving the oral health status of Māori children and young people may likewise lead to a higher proportion of this population visiting oral health providers and therefore maintaining an ongoing demand for a supply of dental therapists, despite improving oral health.
3.5 Use of oral health services
In Australia, modelling a population ’s demand for oral health services ‘is satisfied by the use of services, which can be measured in the dental visits ’ (AIHW Dental Statistics and Research
Unit, 1998, p.103). However, service utilisation is not a proxy for service demand among Māori.
When an accessible and culturally appropriate service becomes available to whānau, utilisation far exceeds Māori historical usage of mainstream services (Broughton, 1995). Noonan and
Evans (2003, p.1030) note what many studies have found, that:
... people seek, and have a preference for, health care providers who are of their own culture and ethnic background ... [and] lack of such providers is a clear barrier to access to quality health care and appropriate utilisation of services.
Māori adults who have not accessed oral health services regularly and/or for some time, and who are at more risk of tooth loss, will attend Māori-initiated dental health programmes in their community (Broughton, 1995). It is therefore plausible that the availability and accessibility of
Māori dental therapists will increase service usage by Māori whānau for their children and young people.
Whānau use of services also offers increased opportunities for oral health promotion that will increase people ’s awareness and expectations. In this way, use of an acceptable oral service will promote more use of that service. Māori will also advertise the service to others through word-of-mouth (Pipi et al, 2003).
Scenario 4. Oral health care from a Māori dental therapist
Culturally acceptable services are catalysts for service use by Māori (Broughton, 1995;
Mauri Ora Associates, 2004). The Māori dental therapy workforce has an important role to play in the provision of these services. The Health Workforce Advisory Committee
(2006), for example, has recommended that increasing the Māori health workforce is a way of easing the shortage of health professionals with an understanding of Māori culture.
While Māori dental therapists are well-positioned to raise the oral health awareness and expectations of whānau, the promotion of healthy oral health behaviour also needs to happen in the community as a means of helping to prevent dental caries (Ministry of
Health, 2006a).
6
Future Directions for a Māori Dental Therapy Workforce
3.6 Oral health service requirements
A commitment to improve the oral health status of M āori children and young people needs to encompass other components of the model described in Diagram 1, namely Māori awareness and expectations, and the provision of accessible oral health services.
Given the combined treatment and prevention system that is currently underway, it is predicted that the oral health status of Māori 0–17-year-olds may improve more than the current predictions in the next eight years. For example, the Lift the Lip intervention trains Well Child/
Tamariki Ora nurses and other non-oral health professionals to assess children ’s oral health needs and refer them to an oral health provider (Ministry of Health, 2008a). If this improvement happens oral health services may be able to cope with the population increase in this age group because, although there will be more of them, their oral health needs will be less (unless counterbalanced by an increase in demand from a shift in normative need, see 3.2 above).
Access to fluoridation is also a key component of the oral health strategy and, if implemented, will complement service provision as a driver of the reduction of Māori oral health disparities for this age group (Ministry of Health, 2006a).
The implication for the Māori dental therapy workforce is that the sooner it has the capacity to respond to Māori oral health need, the sooner it will:
contribute to the oral health status of Māori children and young people
be able to stabilise workforce numbers and productivity in relation to population numbers (without the additional factor of oral health normative need).
This is not to say that the oral health status of Māori children and young people is solely the responsibility of the Māori dental therapy workforce.
Future Directions for a Māori Dental Therapy Workforce
7
4. The supply of Māori dental therapists
This section examines the current and future needs of the Māori dental therapy workforce in an exploration of Scenario 4: that every Māori child is able to receive optimal oral health care from a
Māori dental therapist if they or their whānau choose. Information on the dental therapy workforce more generally is in Appendix B.
What is needed of the Māori dental workforce to fulfil this scenario is examined first for 2006, followed by projected needs in eight years.
4.1 2006 Māori dental therapy workforce
Of the 635 dental therapists holding an APC in 2006 for whom ethnicity data was available,
10.2 percent (N = 65) selfidentified as Māori (Thomson, 2007).
4
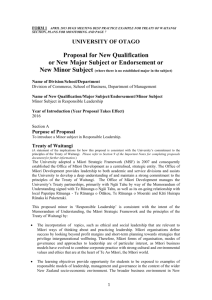
Figure 3: Percentage of non-M āori and Māori dental therapy workforce by age group
Source Thomson (2007, personal communication March 2009)
Figure 3 illustrates that in 2006 over half of the Māori dental therapy workforce (N = 34, 52.3%) was younger than 50 years of age, with over one-third (N = 24, 36.9%) younger than 40 years of age (Thomson, personal communication, March 2009). NonMāori dental therapists, on the other hand, were less well represented in the younger age groups. The main issue for the Māori dental therapy workforce is growing the numbers in the workforce to reflect the Māori population.
In comparison, the main issue for the non-M āori dental therapy workforce is retirement (see
Appendix B).
8
Future Directions for a Māori Dental Therapy Workforce
Scenario 3. Workforce aligned with the population
A basic calculation of Māori being represented in the workforce in proportion to the population of 0 –17-year-olds suggests that at least 20.1 percent of the dental therapy workforce in 2006 should have been Māori; that is, 130 out of 650 dental therapists, or double the number of Māori dental therapists that were in the workforce.
It is also important to consider how many dental therapists there are relative to the population they serve.
In 2006 there were 628 dental therapists who held an APC and were practising as dental therapists (Thomson, 2007). From the 2006 Census data there were 1,081,220 0 –17-year-olds.
Based on these figures there were 58.1 dental therapists per 100,000 population (0 –17 years) in
2006.
5
In the same year there were 65 Māori dental therapists and approximately 256,720 0–17-yearold Māori. There were therefore 25.3 Māori dental therapists per 100,000 Māori population. To increase this ratio to 58.1 Māori dental therapists per 100,000 Māori 0–17-year-olds (as per the general ratio above) would have required 149 Māori dental therapists – that is, 84 more Māori dental therapists than in the 2006 workforce.
The calculation of the need for M āori dental therapists assumes that the workload of Māori dental therapists seeing M āori children is similar to that of dental therapists seeing a general population of children. When productivity (i.e. number of appointments per day) and the need for frequent visits were factored into the calculations (see Appendix C), 149 Māori dental therapists seeing Māori children and young people would have an average productivity of 13.
This was considered high by Māori oral health providers and informants, who suggested a productivity level of 10.9 or lower was more appropriate, given the presenting oral health needs of M āori children and young people. A productivity level of 10.9 would have required 178 Māori dental therapists in 2006.
Scenario 4. Oral health care from a Māori dental therapist
A productivity level of 10.9 would have required 178 Māori dental therapists, or 113 more than in the 2006 workforce.
A reduced productivity level of 8.75 visits per day was recommended by Māori oral health providers to meet demand. This would have required 222 Māori dental therapists in 2006.
Based on these calculations, the 2006 dental therapy workforce could not supply a Māori dental therapist for every Māori child and young person. At the very least 65 more Māori dental therapists were required in the 2006 dental therapy workforce to align the workforce with the
Māori 0–17-year-old population.
4.2 2018 Māori dental therapy workforce
By 2018 the proportion of Māori in the 0–17-year-old population is predicted to increase to
21.2 percent, with the number of 0 –17-year-old Māori predicted to increase by 13.7percent (from
2006) to 291,840. Fifty-two of the 65 Māori dental therapists in the 2006 workforce are predicted to still be in the 2018 workforce.
Future Directions for a Māori Dental Therapy Workforce
9
The dental therapy workforce in 2018 is predicted to be 788 (see Appendix B). Aligning this with th e Māori 0–17-year-old population means that 21.2 percent, or 167, of this workforce should be
Māori.
A ratio of 58.1 Māori dental therapists per 100,000 Māori 0–17-year-olds for this population would require a Māori dental therapy workforce of 170 in 2018.
This predicted supply need does not take into account productivity, which would increase the number of Māori dental therapists needed. In 2018, an average productivity rate of 10.9 would require 208 M āori dental therapists if optimal oral health care for Māori is to be supplied by Māori dental therapists. An average productivity of 12 would require 189 Māori dental therapists, while an average productivity of 15 would require 154.
Scenario 1. Workforce aligned with institutional supply
The projected number of dental therapists in the workforce in 2018, based on institutional supply and taking into account losses from the workforce, is 788 (or a net gain of
138 dental therapists compared to 2006; see Appendix B). For a projected 2018 general population of 0 –17-year-olds (N = 1,091,890) this workforce represents a ratio of
72.2 dental therapists per 00,000 population, an increase of 12 dental therapists per
100,000 population compared to 2006.
Applying the 2006 ratio of 58.1 dental therapists per 100,000 population to the projected nonMāori population in 2018 (N = 800,050) gives a workforce requirement of 465 dental therapists for this population. If the remaining 323 dental therapists projected to be in the
2018 workforce are applied to oral health se rvices for Māori 0–17-year-olds (N = 291,840) the ratio of dental therapists per 100,000 Māori population will be 110.8 in 2018.
While it may not be possible to attain a Māori dental therapy workforce to meet the needs of
Māori 0–17-year-olds by 2018, the projected 2018 dental therapy workforce has the potential to provide optimal oral health care for Māori 0–17-year-olds (Scenario 2).
4.3 Assumptions
The assumptions that underpin Scenario 1 and the projections for a Māori dental therapy workforce to meet the oral health needs of Māori 0–17-year-olds are specified below.
That Māori dental therapists will be practising only with 0–17-year-olds
Many (if not most) of the dental therapists working for iwi providers have their adult scope and work in oral health teams (Informant 6). New graduates are also able to practise with adults as dental hygienists. In both cases work with adults potentially detracts from the sole focus on 0 –17-years-olds that is assumed in the supply calculations and would therefore increase the needed su pply of Māori dental therapists.
That Māori dental therapists will work with Māori 0–17-year-olds
Some Māori dental therapists will choose not to work with Māori, 6 or they may choose to work with Māori but be overwhelmed by non-Māori wanting to access their service and effectively shutting many Māori out (Informant 5). If this second assumption does not hold the needed supply of Māori dental therapists increases.
10
Future Directions for a Māori Dental Therapy Workforce
That some Māori children and young people will see non-Māori dental therapists
Not every Māori child or young person may want to see a Māori dental therapist. It may also be that some nonMāori dental therapists will be able to provide culturally competent oral health care. If this third assumption is correct then the needed supply of Māori dental therapists decreases. The provision of culturally competent oral health care by nonMāori dental therapists underlies the realisation of Scenario 2 (also see the boxed section about Scenario 1).
That some Māori children and young people will see other oral health professionals
The productivity calculations are based on 50 percent of Māori 13–17-year-olds receiving oral health care from a Māori dental therapist. If more young people, and some children, opt out of oral health care from a Māori dental therapist then the needed supply of Māori dental therapists decreases.
That Māori oral health therapists with a dual qualification in dental therapy and dental hygiene will work as dental therapists
If a proportion of dual qualified Māori dental therapists choose to work partially or fully as dental hygienists then the needed supply of Māori dental therapists increases.
7
Some of the assumptions, if correct, add to the supply demands on the Māori dental therapy workforce and some subtract from these demands. On balance the premise appears to be a good starting point for analysing the current and future supply of Māori dental therapists.
4.4 Summary
In 2006 there were 65 Māori dental therapists. At least 65 more Māori dental therapists were needed to reflect t he proportion of Māori 0–17-year-olds in the 2006 population. When the oral health status of Māori 0–17-year-olds was taken into account in adjustments that lowered productivity expectations this rose to between 84 and 252 additional Māori dental therapists being needed just to serve the 2006 population of Māori 0–17-year-olds.
By 2018 the projected workforce need is for between 174 and 208 additional Māori dental therapists, based on the assumption that 52 of the Māori dental therapists in the workforce in
2006 will still be in the workforce in 2018. While it may not be possible to meet this projected need with Māori dental therapists, the projections for the dental therapy workforce as a whole suggest that it will have the potential to provide optimal o ral health care to Māori 0–17-year-olds.
Future Directions for a Māori Dental Therapy Workforce
11
5. Māori and secondary school science
The next two sections examine educational pathways into dental therapy. The model guiding the present analysis is described in Ratima, Brown et al (2007) (Diagram 2).
Diagram 2: M āori health and disability workforce development pathway
Source Ratima, Brown et al, 2007
In 2007 18 percent of Māori secondary school leavers had achieved qualifications that allowed them to study at university, an increase of 11 percent from 2002 (Ministry of Education, 2009a).
This increase does not bode well for the health sciences, however, as the proportion of secondary school students participating and achieving in science remains low.
This section examines Māori students’ participation in, and attainment of, secondary school science subjects and uses current data to predict future participation and attainment. Some of the barriers to, and facilitators of, Māori participation and attainment in secondary school science are then examined, including those occurring prior to secondary school. Section 7 examines the role of the tertiary education institutes offering dental therapy education.
5.1 Māori student participation in science
The participation 8 of Māori students in science at Year 11 increased from 66.3 percent
(N = 5950) in 2004 to 71.5 percent (N = 8282) in 2009. The comparable participation rate for nonMāori students increased from 84.2% to 86.0% (see Figure 4). The upward trend in the participation of Māori students is predicted to continue, with the proportion increasing to
75.6 percent in 2013 and to 79.8 percent in 2018.
9 While the 2018 prediction for Māori participation is below the 90.1 percent participation predicted for nonMāori students, the gap between Māori and non-Māori participation is predicted to narrow.
12
Future Directions for a Māori Dental Therapy Workforce
Figure 4:
Māori and non-Māori participation rate (percentage) in Year 11–13
NCEA science subjects, 2004 –2007, and predicted participation in
2013 and 2018
100%
90%
80%
70%
60%
50%
40%
30%
Key
Māori Year 11
Māori Year 12
Māori Year 13
Non-Māori Year 11
Non-Māori Year 12
Non-Māori Year 13
20%
10%
0%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Year
Source 2004
–2007 rates, Ministry of Education and 2008–2018 predicted rates (2008–2018), Research
Evaluation Consultancy 8
The participation of Māori students in Year 12 science subjects increased modestly from 2004
(31.9%, N = 1871) to 2009 (32.2%, N = 2757) and this increase is predicted to continue in 2013
(32.6%) and 2018 (33.1%). Declines in nonMāori participation in science, from 54.4 percent in
2004 to 52.5 percent in 2009, are predicted to continue in 2013 (50.5%) and 2018 (48.7%). Both trends contribute to the predicted reduction in the gap between M āori and non-Māori participation by 2018.
The percentage of Māori students participating in Year 13 science declined from 24.6 percent
(N = 827) in 2004 to 23.2 percent (N = 1008) in 2009. This decline is predicted to continue, with the proportion dropping to 21.7 percent in 2013 and 20.3 percent in 2018. This decline was also reflected in nonMāori student participation, which decreased from 47.8 percent (N = 11,875) in
2004 to 39.8 percent (N = 12,759) in 2009. The predicted participation rate of nonMāori students in 2018 (26.2%) is not much higher than the predicte d Māori participation rate
(20.34%).
The participation rate of Māori students has been much higher at Year 11 than at Years 12 and 13. Assuming that the same cohort of Māori students were in Year 11 in 2007, in Year 12 in
2008, and in Year 13 in 2009 , then the Māori participation rate drops by two-thirds from Year 11
(69.1%) to Year 13 (23.2%) (Table 2). The nonMāori participation rate across the same period also drops, but only by slightly over half (from 85.3% to 39.8%).
Future Directions for a Māori Dental Therapy Workforce
13
Table 2:
Participation of Māori and non-Māori student cohort in science,
Years 11 –12, 2007–2009
Māori
Non-
Māori
Number
Percentage
Number
Percentage
2007
Year 11
7,734
69.1
38,592
85.3
2008
Year 12
2,606
32.0
20,564
51.9
2009
Year 13
1,282
23.2
12,759
39.8
Source Ministry of Education, Unpublished data, 2008
5.2
Māori student attainment
10
in science
Māori student attainment rates in Year 11 science were around 40 percent during 2004 to 2009.
It is predicted tha t in 2013 the attainment rate for Māori students will be 42.1 percent, with a slight increase to 43.5 percent in 2018 (see Figure 5).
11 NonMāori student attainment rates also remained reasonably static in the 2004 –2009 period at around 63 percent. A similar level of attainment is predicted in 2013 (62.7%) and 2018 (62.6%).
The attainment of Māori students in Year 12 science increased from 38.5 percent (N = 721) in
2004 to 42.3 percent (N = 1165) in 2009. This increase is predicted to continue in 2013 (45.9%), with a further increase to 49.2 percent predicted in 2018. NonMāori attainment rates in Year 12 also increased from 63.4 percent in 2004 to 65.7 percent in 2009. This increase is predicted to continue in 2013 (66.9%), with an attainment rate of 68.1 percent predicted in 2018.
Year 13 Māori student attainment in science in 2004 was 42.8 percent (N = 354). This was increasing to 2008 (45.1%) and then dropped back in 2009 (41.2%). It is predicted to hold steady at 42.5 percent in 2018. The number of Māori students attaining Year 13 science by
2018 is still predicted to remain below 1000. The gap between Māori and non-Māori student attainment at Years 11 and 12 is predicted to reduce by 2018 and remain static at Year 13.
14
Future Directions for a Māori Dental Therapy Workforce
55%
50%
45%
40%
Figure 5:
Māori and non-Māori attainment (percentage) in Year 11–13 NCEA science subjects, 2004 –2007, and predicted attainment in 2013 and
2018
70%
65%
60%
Key
Māori Year 11
Māori Year 12
Māori Year 13
Non-Māori Year 11
Non-Māori Year 12
Non-Māori Year 13
35%
30%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Year
Source Ministry of Health (2009)
If, as with participation, it is assumed that the data allows a cohort of students to be followed through Years 11, 12 and 13 (2007 –2009), then the increase in the attainment rate of Māori students over these years (from 40.0% at Year 11 to 41.2% by Year 13) needs to be seen within the context of the drop in the number of Māori students who attain science subjects (down from
3093 in Year 11 in 2007 to 528 in Year 13 in 2009) (Table 3).
In addition, of the 7734 Māori students participating in Year 11 science in 2007 (see Table 2),
6.8 percent (N = 528) attained Year 13 science in 2009. The comparable figure for nonMāori students was 21.4 percent. (These proportions were slightly down on the 2004 –2006 cohort percentages of 7.0% for Māori and 22.0% for non-Māori.)
Table 3: Attainment of Māori and non-Māori student cohort in science,
Years 11 –13, 2007–2009
Māori
NonMāori
Number
Percentage
Number
Percentage
Source Ministry of Health (2009)
2007
Year 11
3,093
40.0
23,931
62.0
2008
Year 12
1,101
42.2
13,421
65.3
2009
Year 13
528
41.2
8,241
64.6
Future Directions for a Māori Dental Therapy Workforce
15
5.3 Ensuring success in science
The Health Workforce Advisory Committee (HWAC) (2006) summed up the consequences of
Māori secondary school student engagement with science by stating that ‘many Māori are prevented from entering the health professions as they do not have high school qualifications ’.
Māori secondary students need to be encouraged to participate in science at secondary school, with the promotion of science beginning long before they get to secondary school. There is also an urgent need to retain those who are participating in Year 11 so that they continue studying science.
The key informants in the Rauringa Raupa study (Ratima, Brown, et al, 2007) identified the lack of support for Māori students and their whānau within the current educational system as a major barrier to Māori students continuing to tertiary education in a health profession. This included
Māori students not being encouraged to study science at school, so that they end up thinking of science as uninteresting and irrelevant.
12
One potential solution rests with Te Kotahitanga, a research and professional development programme aiming to improve the educational attainment of Māori students in mainstream secondary schools. Through training and feedback teachers become more culturally aware, learning how they and their students can co-construct a learning environment (Bishop,
Berryman, Cavanagh & Teddy, 2009).
The components of successful recruitment and retention interventions that encourage and support Māori students to study science, and that interest them in health careers, include:
the promotion of science and careers in health to both students and their whānau and community 13
the introduction of role models and mentors 14
academic preparation, including the provision of career advice and study pathways 15
maintaining and stressing economic incentives 16 (Ratima, Brown, et al, 2007, p.180;
HWAC, 2006, p.4).
The provision of good quality oral health care to pre-secondary school students may be an important motivator for students subsequently thinking about a career in oral health therapy.
Veal et al. (2004, p.938) found that minority students ’ decisions about applying to dental schools in the United States ‘hinged on them having had early and frequent exposure to dentistry and dentists in practice ’.
The Health Workforce Advisory Committee (2006) endorsed the revision of the science curriculum so that it was more relevant for communities and thereby more interesting as well as cross-disciplinary. This included recommendations for:
more individual student choice over the modules that make up the science courses
links with the Ministry of Research, Science and Technology (MoRST) and organisations to make science classes more interesting e xtension of Te Kotahitanga Programme to improve teaching of Māori students, including recognition of students ’ ‘cultural capital’ and the notion of reciprocal learning whereby the teacher also learns from the students use of asTTle (Assessment Tools for Teaching and Learning – He Pūnaha
Aromatawai mō te Whakaako me te Ako) to assess and address individual student weaknesses.
16
Future Directions for a Māori Dental Therapy Workforce
5.4 Summary
Over the next eight years the number of Māori students participating in science at secondary school will increase as the population in this age group increases. The participation rate of these students in Years 11 and 12 science will increase and the gap in participation between
Māori and non-Māori students will reduce for all years. However, the drop-out rate in Māori participation in science as students move from Year 11 to Year 13 is predicted to increase, largely due to a large decrease in the participation rate as students move from Year 11 to 12, and declining participation rate at Year 13.
M āori student attainment in science in 2004 through 2009 has been less than 50 percent at all levels. While attainment is predicted to increase in the next eight years, the absolute number of
Māori students is predicted to remain low, with less than 1000 Māori students predicted to attain
Year 13 science in 2018. Approximately one in five nonMāori students who participated in science at Year 11 in 2005 attained NCEA science at Year 13 in 2007. The comparable figure for Māori was less than one in 14 students. While the first issue is encouraging more Māori students to participate in science, students who do participate also need to be nurtured and taught well so that they go on to achieve.
All the pointers are that the science curriculum may well have to become more relevant and interesting for Māori students and their whānau. It is predicted that this will increase the motivation of Māori students to participate in science at secondary school as well as supporting their attainment in science. This needs to be enhanced by good career advice alongside individual assessment and remediation. Role models remain important throughout schooling and, in the case of dental therapy and stepping students onto a career pathway in oral health, the provision of good quality oral health care may well be pivotal.
Future Directions for a Māori Dental Therapy Workforce
17
6 Tertiary education in dental therapy
A bachelors degree is now the minimum qualification needed for someone new to the field to work as a dental therapist.
17 Auckland University of Technology (AUT) and the University of
Otago (Otago) each offer a three-year bachelors degree that incorporates both dental therapy and dental hygiene education. The AUT Bachelor in Health Science in Oral Health began in
2006; the Otago Bachelor of Oral Health began in 2007. The course at AUT has a community focus, with the utilisation of community clinics within Auckland for educational purposes. The focus at Otago is more on the integration of oral health therapy with other disciplines in dentistry
(DTTAG, 2004). The two universities are also striving to collaborate more.
Despite these differences, the teaching philosophy at both institutions has a focus on students developing and attaining proficiency and competence, so that they meet the required standards of the dental therapy health profession (DTTAG, 2004, p.4).
This section looks at the recruitment and retention of Māori students in the bachelors programmes offered by AUT and Otago.
6.1
Recruiting Māori students
Over the past ten years Māori participation in tertiary education has increased at twice the rate of nonMāori participation, growing from around 7 percent in 1998 to nearly 20 percent of Māori aged 15 years and over participating in some form of tertiary education in 2004 (Figure 6). The decline in Māori participation that began in 2006 and continued through to 2008 has been attributed to a reduction in certificate level programmes (Ministry of Education, 2008).
One of the main factors in the growth of Māori participation in tertiary education was increased
Māori enrolments at wānanga, especially Te Wānanga o Aotearoa (Ministry of Education, 2005).
M āori participation rates in 2007 were highest at the sub-degree level, and Māori students also have an historically high progression rate from certificate level courses to higher-level qualifications (Ministry of Education, 2008). Students in sub-degree tertiary study are therefore a pot ential pool of Māori who can be encouraged and supported to enter into health degree programmes. One impediment to degree-level studies is that M āori students do not leave secondary school with good levels of participation and achievement rates in science. W ānanga therefore may be well-placed to offer bridging courses for students to dental therapy programmes at either AUT or Otago, and the establishment of a wānanga-based oral therapy programme should not be overlooked as wānanga are already delivering some health courses and are an accessible tertiary provider for Māori.
18
Future Directions for a Māori Dental Therapy Workforce
Figure 6: Age-standardised participation rates in tertiary education per 100 population aged 15 years and over by ethnic group, 1994 –2008
Source Ministry of Education (2009b)
HWAC (2006, p.11) also argues that foundational courses, including those offered by the universities themselves, enable Māori students (mature or school leavers) to gain necessary skills and knowledge before commencing tertiary courses. There is a risk, however, that by prolonging people ’s education, foundational courses also prolong their time away from home and increase their student debt. Offering foundation or bridging courses locally for people may overcome geographical barriers and allow people to obtain the necessary prerequisites (i.e.
NCEA level 2 English and biology) to apply for entry into a dental therapy programme. An informant also suggested that people could obtain these prerequisites ‘for free’ by returning to high school (Informant 5).
Finding out about these options and getting good career advice can be barriers for mature students (Ratima, Brown et al, 2007). HWAC (2003, p.14) recommended that DHBs take a lead in promoting health careers and ‘... consider second-chance health education initiatives, including work experience and internships for Māori’.
The DHBNZ (2004, p.20) review also described workforce issues that include ‘younger people
[not appearing] to find dental therapy an attractive career option ’. However, this does not seem to be the experience of AUT and Otago. It used to be older women who entered the profession, but now the average age of those in the Otago programme is around 26 years (Informant 6).
18
In 2007 AUT accepted 30 students into its Bachelor in Health Science in Oral Health programme, two (6.7%) of whom were Māori (see Table 4). The number of students accepted in 2008 rose to 43, three (7.0%) of whom were Māori. In 2009 three (7.1%) of the 42 students accepted were Māori.
In 2009 AUT introduced a new admissions scheme to replace a system whereby students were given places in health courses before they enrolled. Students all did a semester of health papers and then applied (Informant 4). Of the 272 applicants, AUT selected 42 (Table 4).
Those accepted into the Bachelor of Health Science in Oral Health then start the oral health papers in the second semester. The only selection criteria in the AUT calendar (2008, p.137) is that applicants ‘must be capable of meeting HPCA Act requirements, [and have] police clearance ’. Difficulties administering the new admissions scheme mean that in 2010 students for the Bachelor of Health Science in Oral Health will be selected before the beginning of semester one.
Future Directions for a Māori Dental Therapy Workforce
19
Table 4:
Recruitment of Māori students into the AUT Bachelor in Health Science in Oral Health programme
Year
2007
2008
2009
Total
Applications
Māori
Total
11
10
14
35
204
282
272
758
First year enrolments
Māori
Total
2
3
3
8
30
43
42
115
Degree completions
Māori
Total
4
5
3
12
13
24
29
66
Source Information supplied by AUT.
Note: AUT has found that places in their Bachelor in Health Sciences in Oral Health programme are frequently offered and not accepted as students have applied for, and subsequently accepted, a place in another health programme (e.g. nursing, physiotherapy).
AUT gives priority to Māori and Pasifika students applying for entry into its Bachelor in Health
Science in Oral Health programme. The university finds that the hardest thing is recruiting Māori into the course; once they are in, they are fine (Informant 7). The AUT Health Faculty has connections with schools and the Oral Heath Department is actively involved in campus tours and educational sessions.
AUT is also committed to second chance education for mature students (Informant 4). Students who may not immediately be eligible or confident enough to enter the bachelors degree programme can begin with AUT ’s foundational Health Sciences Certificate programme.
Otago has capacity for 42 students in its Bachelor of Oral Health programme and 34 were accepted in 2007, with this increasing to 41 students in 2009 (Table 5). Students entering the oral health therapy programme at Otago in 2009 ranged in age from school leavers to students in their 40s (Informant 10). The students start their clinical oral health paper at the start of their first year, and start treating patients in the first semester of their second year.
Admission to the Bachelor of Oral Health at the University of Otago (2009 information from website) requires students to have obtained a satisfactory level in NCEA level 2 Biology and
NCEA level 2 English (or NCEA recognised equivalent). In 2009 there were five Māori students in the Otago programme (two in third year, one in second year, and one in first year)
(Informant 10).
Māori students who have done the 12-month foundation course at Otago have always been successful in getting into the discipline of choice (Informant 5). In 2010 Otago begin their
Tū Kahika programme, ‘a Health Sciences programme run within Foundation Year, which will prepa re Māori students academically for their first year of tertiary study and future career in
Māori health’ (University of Otago, 2009). Students who complete Tū Kahika can apply for direct admission into the Bachelor of Oral Health.
20
Future Directions for a Māori Dental Therapy Workforce
Table 5: Recruitment of
Māori students into the Otago Bachelor of Oral Health programme
1
Year
Total
N
Enrolments
Māori
N %
Total
N
Degree completions
Māori
N %
2005
2006
2007
2008
92
107
73
63
7
7
6
3
7.6
6.5
8.2
4.8
34
41
45
1
1
3
4
0
2.9
7.3
8.9
0.0
Source University of Otago, personal communication
Note : Pre-2007 data is for students enrolled in dental hygiene and dental therapy courses.
Nationally, the newly implemented Kia Ora Hauora – Māori Health Careers Programme aims to recruit 1,000 Māori into health career pathways by 30 June 2012. ‘The Programme will offer a comprehensive and coordinated suite of information and support services, at both national and regional levels, dedicated to assisting more Māori into their preferred health career pathway’
(National Coordination Centre & Regional Coordination Hubs, 2009, p.4).
6.2
Retaining Māori students
Jefferies (1998) listed inadequate school qualifications, negative school experiences, unwelcoming tertiary environments, and financial difficulties as key barriers to Māori participation in tertiary education. The Ven Turi Hollis (2000), University of Canterbury chaplain, added homesickness, loss of whānau, student debt, and the challenge of tertiary education to students’ cultural identity. An additional barrier for mature students can be isolation because of their living arrangements.
They can get so easily lost ... [and support is] probably [needed] more for grownups in different ways. They often don ’t live in hostels or in flats; they live in studio rooms and things like that so they can be really isolated (Informant 10).
Since the early 1990s the Hauora Māori Scholarship Programme has provided some financial assistance for students undertaking tertiary-level health programmes. Students need to be committed to Māori health and have whakapapa/cultural links to Māoridom (Ratima, Waetford, et al, 2007). From 1997 to 2005 there were at least 36 Hauora Māori Scholarship recipients in the Dental category. Of these recipients, 20 held an APC in 2006, four of whom were dental therapists (Ratima, Waetford, et al, 2007).
Other, non-loan study assistance is also available (HWAC, 2006). If students are aware of this assistance and know how to access it then the cost barrier to studying can be reduced.
Institutional commitment from tertiary providers is also important.
According to key informants important barriers to Māori participation in health programmes are; a lack of value or recognition of Māori approaches in tertiary institutions, lack of or limited access to programmes delivered in a way that is appropriate to Māori, lack of or inadequate Māori content in programmes, and the low numbers of Māori students in health programmes to provide peer support
(Ratima, Brown, et al, 2007, p.73).
Future Directions for a Māori Dental Therapy Workforce
21
An informant in the present study reported that Otago has a good Māori student support system
(Informant 10). There is a mihi whakatau for all new students. Students in the Oral Health
Therapy programme do a compulsory firstyear paper in Māori society and then they get aspects of oranga niho (Māori oral health) in the second and third years (Informant 5). Otago also has an out-placement programme for students in their third year whereby they can return home and work alongside a local dental therapist (Informant 10).
Students at AUT are able to study Māori health at each year of the course, with this being compulsory for all students in the first year (Informant 4). Papers offered by AUT include:
Māori Health Promotion
Māori Health, Development and Environment
Applied Māori Mental Health
Health and Environment.
AUT students can do the course part-time but then it is harder to for them to get a student loan
(Informant 7). Many of the students also do placements in Māori communities (Informant 7).
Academic help and study support are offered by Te Tari Awhina, the Learning Development
Centre at AUT. In addition Te Tar i Takawaenga Māori, Māori Student Support, aims to both recruit and support Māori at AUT.
T here is a lot of support at AUT for Māori students. Once they come, they don’t usually drop out (Informant 7).
The first dual-qualified (in both dental therapy and hygiene) oral health therapists graduated from
AUT in 2008, while the first cohort of students will graduate from Otago in 2009. In 2008 five
(20.8%) of the AUT graduates were Māori, while in 2009 three (10.3%) of the graduating class of
29 students were Māori (see Table 4).
[The new programme] has given those graduates a really valuable skill [that ’s] sought after anywhere in the world (Informant 6).
6.3 Summary
At the tertiary level the Tertiary Education Strategy 2007 –2012 is the basis of the relationship between health, its workforce, and the providers of tertiary education (Ministry of Health &
DHBNZ, 2007). A key priority area in this strategy is the reduction of skills shortages through building relationships with health sector stakeholders to understand how to improve the relevance of tertiary education.
The relationship between the health and education sectors is fundamental to effective workforce development. The education sector is a major supplier of our health workforce. Courses and learning provided in tertiary education institutes must be responsive to the workforce needs of the health sector (Ministry of Health & DHBNZ, 2007, p.5).
Both Otago and AUT now offer a three-year bachelors degree that combines dental therapy and dental hygiene education. Both institutions provide support for Māori students, although AUT has experienced difficulty in recruiting Māori students into their programme. The number of
Māori students in the Otago programme is also small. This suggests that clearer pathways into the programmes need to be facilitated for Māori. The promotion of dental therapy as a career by current Māori students and by career role models are reasonably straightforward options.
The tertiary institutions themselves are also working to make their environment more userfriendly for Māori students. The programmes include Māori content and Māori staff, and students in the AUT programme can opt into a Māori health stream during their course. Course placements within communities are also available.
22
Future Directions for a Māori Dental Therapy Workforce
Second chance entry into the oral health therapy programme is encouraged by both AUT and
Otago. Other options that allow mature students to gain entry qualifications without leaving home should also be explored, alongside raising the awareness of such students of the financial assistance and study options that are available to them.
A potential barrier to students entering into oral health therapy courses is its attractiveness as a career option. Overcoming this requires at least a dual approach of promoting oral health therapy as a career to potential students and ensuring that the working conditions within the profession itself remain attractive in comparison to other careers that have similar training requirements.
Future Directions for a Māori Dental Therapy Workforce
23
7 Dental therapy work environment
In 2004 the Health Practitioners Competence Assurance Act 2003 (HPCA Act 2003) removed the restriction on dental therapists only being able to be employed in the public service (DTTAG,
2004). Dental therapists are now able to be located within primary health organisations and
Māori health providers, and they can treat patients in private dental practice. The scope of practise for dental therapists has also changed and they can now provide oral health services for children and young people up to the age of 17 years (DHBNZ, 2004).
19 Dental therapists can also practise with adults if they acquire the extra training needed for an adult scope.
20
The AUT and Otago programmes are producing graduates with a dual qualification in dental therapy and dental hygiene. There is potential for these new oral health professionals to be seen as quite distinct from the existing dental therapy workforce, even when they choose to practise as dental therapists.
21
These factors all impact on the working conditions of the Māori dental therapy workforce. This section deals in particular with how the transition of new Māori graduates into the workforce can be supported, and how the working environment for dental therapists can be made more attractive for Māori dental therapists.
7.1 Transition to work
The supported transition of new Māori oral health therapy graduates from study into the workforce is a crucial period in workforce retention and can be supported by the following initiatives (cf. Ratima, Brown et al, 2007).
Mentoring through the transition from study to work, with opportunities for graduates to align their interests with their area of work.
Career counselling of both career options and future education planning.
22
Access to Māori health professional networks. Te Ao Marama (the New Zealand
Māori Dental Association) is inclusive of all Māori delivering oral health care (Mauri
Ora, 2004).
7.2 Working environment
The DHBNZ (2004) review predicted that when dental therapists were freed up to practise privately they would likely choose some mix of private and public practice. The Queensland experience was that initially the swing was toward private practice but this settled with a balance of public and private (Informant 6). The first graduates from AUT only graduated in 2008, and the first from Otago will graduate in 2009, so it may be some while before it is known how the private-public balance will settle here for new graduates (Informant 4). DHBNZ (2004, p.6) anticipated the potential pull of private practice and recommended that ‘DHBs implement a national review of dental therapy salary and conditions of employment ’.
23
An informant also commented that there is now a push for better employment conditions for dental therapists (Informant 3). This may remedy the survey findings from Ayers et al (2007) that younger dental therapists were more likely to report an interest in private practice, and that overall dental therapists were less than satisfied with their remuneration.
This section examines some of the aspects of the working conditions of dental therapists.
24
Future Directions for a Māori Dental Therapy Workforce
7.2.1 Isolation
DHBNZ (2004) identified the need for the revitalisation of school dental clinics to make them
‘safe, modern and functional’. The introduction of dental assistants to work alongside dental therapists went some way to addressing the isolation of sole operators (DTTAG, 2004, p.15).
The linking up of school dental clinics and mobile clinics in community-based oral care networks may go some way to addressing concerns about isolation and support. There are also calls for oral health and primary health to sit along one another.
They ’re now ... working with a team. They get more support, the job’s more enjoyable, they get more feedback .... There ’s mentorship. Things are changing and I think we ’ll also see those changes occur with [the oral health] of our children
(Informant 10).
Dental therapists who felt valued as members of the dental community were four times more likely to experience career satisfaction than those who did not feel this way (Ayers et al, 2007).
7.2.2 Pay
In the 1990s the pay parity that dental therapists had with teachers disappeared, along with nationally consistent employment conditions. In 2004 DTTAG reported that dental therapists ’ annual salaries were approximately $10,000 behind equivalent teacher salaries, identifying this as a risk to the retention of dental therapists in the public sector (and possibly the recruitment of
Māori into the profession).
24
7.2.3 Career incentives
In Tasmania dental therapists can progress to being senior dental therapists or move on to oral health therapist positions that are about the coordination of state-wide dental health initiatives
(Tasmanian Department of Health and Human Services, 2003). While there are career options here (e.g. dental managers) they are not necessarily utilised well 25 (Informant 6). Another informant saw the need for more dental therapists to gain postgraduate qualifications so that research and/or teaching positions became a career pathway (Informant 6).
26
Dental therapists also need professional development hours each year in order to maintain their practise certificate (Informant 6). This can be a sticking point for Māori working for mainstream health providers as they may not be given the leave and support to undertake professional development (Informant 2). An informant did, however, think that DHBs were becoming much better employers (Informant 4).
7.2.4 Māori preferred-employer criteria
The Health Workforce Advisory Committee (2002) set out Māori preferred-employer criteria, an adaptation of the magnet hospital concept, as a way for DHBs to progress the Māori health workforce (also see Ratima, Brown et al, 2007). This includes the development of Māorispecific employment pathways. The Māori preferred-employer criteria include having:
a philosophy that supports Māori aspirations, including Treaty of Waitangi responsibilities
health interventions that recognise the importance of whānau and community context
career pathways
‘training programmes to meet cultural, professional and Māori health development needs ’ a whānau-friendly environment
support for staff wellness
Future Directions for a Māori Dental Therapy Workforce
25
Māori participation at all levels active employer involvement in the community.
27
7.3 Summary
The HPCA Act 2003 brought a change to the profession which, for the first time, was able to practise beyond the confines of the public service. Combined with the new training programmes at AUT and Otago, this has put pressure on employers to improve the working conditions of oral health professionals so that graduates will be attracted to practising as dental therapists within the public service. Support for new Māori graduates can also be found through membership in professional bodies such as Te Ao Marama and from other, additional, mentoring and career support.
The working conditions of dental therapists include the opportunity to:
work in teams, rather than in isolation be paid commensurate with their qualifications
be supported in their professional development.
An important component of the working environment for Māori dental therapists includes a workplace that acknowledges and supports Māori aspirations and encourages Māori to participate at all levels of the organisation.
28
26
Future Directions for a Māori Dental Therapy Workforce
8 Overall summary and recommendations
The aim of the present project was: to collate information on the status of the Māori dental therapy workforce, and analyse the needs of the Māori dental workforce over the next eight years.
8.1 Four future scenarios
Each of the four scenarios explored in the present paper is summarised below (Table 6). It is unlikely that a requirement for optimal oral health care for Māori children and young people will be able to be delivered by a Māori dental therapy workforce by 2018 (Scenario 4) or that the ethnic composition of the workforce will align with that of the population it serves (Scenario 3). It is more probable that optimal health care for Māori 0–17-year-olds will need to be delivered by both Māori and non-Māori dental therapists. The current projection for the growth in the overall dental health workforce suggests that there is potential for this to occur if services and the workforce are accessible for Māori (Scenario 2). This should not, however, reduce a commitment to building the Māori dental therapy workforce as a key mechanism for reducing the oral health disparities experienced by this age group.
Increasing Māori participation in both the regulated and unregulated workforce will build a representative, culturally safe and competent national health and disability workforce that will lead to optimal health outcomes for all New Zealanders (Ministry of Health, 2008b, p.4).
8.2 Policy implications
The supply of Māori dental therapists is crucial to the development of acceptable oral health services for Māori children and young people. This supply need is currently urgent and predicted to increase in the next eight years. In order to accelerate the supply of Māori dental therapists:
Māori children and young people need to experience good oral health secondary schools need to suppo rt the achievement of Māori students in science
dental therapy as a career option needs to be attractive in terms of remuneration and working conditions
t he number of Māori accepted into dental therapy programmes needs to rise dramatically.
There is also potential for the projected general dental therapy workforce to provide optimal oral health care to Māori 0–17-year-olds. For this to occur non-Māori dental therapists need to be able to provide a culturally competent oral health care service that is committed to alleviating what Broughton and Koopu (1996, p.5) describe as ‘long periods of total neglect’. This aligns with the oral health strategy ’s (Ministry of Health, 2006a, p.5) principle that ‘a robust and appropriately trained workforce provides a high-quality service ’.
Future Directions for a Māori Dental Therapy Workforce
27
Table 6: Future scenarios for the dental therapy workforce, 2018
Scenario Workforce requirement(s)
1. Growth in the oral therapy workforce that aligns with what the current institutions can supply
The estimated dental therapy workforce in 2018, based on projected losses due to workforce retirements and gains from graduates entering the workforce, is 788 dental therapists.
Based on 2006 percentages, approximately 10 percent of these dental therapists will be Māori (i.e. 79). If this includes 52 from the 2006 workforce, then the institutions need to graduate between 2 and 3 Māori students each year from 2007 to 2017. This is in line with current institutional data.
2. Every Māori child receiving optimal oral health care, with a growing Māori workforce contributing to this service provision
3.
The proportion of Māori in the oral health therapy workforce aligning with the proportion of the
0
–17-year-old population that is Māori
Applying the 2006 ratio of 59.6 dental therapists per 100,000 population indicates that, in 2018, 465 of the projected workforce of 788 dental therapists (see Scenario 1) will be needed to supply oral health care to the nonMāori 0–17-year-old population.
Committing the remaining 323 dental therapists to the provision of oral health services to Māori will give a ratio of 110.8 dental therapists per
100,000 Māori 0–17-year-olds. This ratio can potentially supply optimal oral health care to Māori 0–17-year-olds.
The projected 0
–17-year-old Māori population in 2018 is 291,840, or
21.5 percent of the total projected population in this age group.
Based on the general dental therapy workforce projection in Scenario 1,
167 of the 788 dental therapists in 2018 will be Māori if the workforce aligns with the population.
It is predicted that 52 of the 2006 Māori dental therapy workforce will still be working in 2018.
Therefore 115 new Māori dental therapists will be needed
– that is, just over 10 Māori graduates each year from 2007 to 2017.
4.
Every Māori child being able to receive optimal oral health care from a
Māori dental therapist if they or their whānau choose
For the optimal oral health care for Māori 0–17-year-olds to be provided by
Māori dental therapists in 2018 between 10 and 13 new Māori dental therapists would need to enter the workforce each year from 2007 to
2018.
The following policy implications arise from the present analysis of the Māori dental therapy workforce.
1. Māori children and young people urgently need good oral health care. DHBs need to hold all oral health providers, including themselves, accountable for the oral health of Māori children and young people. This may mean, for example, cultural competency training for nonMāori oral health professionals, the purchasing of more Māori oral health services, and the provision of oral health services at times and in places that are most accessible for Māori whānau.
2. Māori secondary school student science attainment needs to increase to at least
20 percent of those participating in Year 11 science, attaining Year 13 science. While general support, monitoring and individualised pathways for Māori secondary school students may gain some traction, investment in the professional development of teachers
(Te Kotahitanga) is also showing promise. In addition the science curriculum itself may need to be made more relevant to Māori students and their whānau, offer students more individual choice, be made more interesting and take a more cross-disciplinary approach.
28
Future Directions for a Māori Dental Therapy Workforce
3. The number of Māori training to be dental therapists needs to increase. Both the
University of Otago and AUT need to actively recruit Māori students into their programmes. Each programme needs to commit to enrolling at least 8 –10 Māori dental therapy students each year for the next six years if the 2018 dental therapy workforce is going to have a representative number of Māori dental therapists – that is, a Māori dental therapy workforce that is proportionate to the 0 –17-year-old Māori population in 2018.
This recruitment should be actively supported by scholarships for these students.
4. The provision of other tertiary options for educating Māori dental therapists should be explored, including the funding of a programme developed by a wānanga and/or the provision of scholarships so that Māori students can train in Australian programmes.
5. The DHBs need to make the working conditions and remuneration of dental therapists in the public service more attractive. For Māori dental therapists this also means making the workplace supportive of them bein g Māori and practising dental therapy in a way that is compatible with this.
Future Directions for a Māori Dental Therapy Workforce
29
References
AIHW Dental Statistics and Research Unit. 1998. Australia ’s Oral Health and Dental Services . AIHW
Cat.No.DEN 13. Adelaide: AIHW Dental Statistics and Research Unit, The University of Adelaide
(Dental Statistics and Research Series No.18).
Auckland University of Technology. 2008. AUT 2009 Academic Calendar . Auckland: Auckland
University of Technology.
Australian Health Minister
’s Advisory Council. 2001.
Oral Health of Australians: National planning for oral health improvement . Adelaide: South Australian Department of Human Services.
Ayers KM, Meldrum A, Thomson WM, et al. 2007. The working practices and career satisfaction of dental therapists in New Zealand. Community Dental Health 24: 257 –63.
Bishop R, Berryman M, Cavanagh T, et al. 2009. Te Kotahitanga: Addressing educational disparities facing Māori students in New Zealand. Teaching and Teacher Education 25(5): 734 –42.
Broughton J, Koopu P. 1996. Dental Health S ervices and Māori People
. Dunedin: Te Roopu Rangahau
Hauora Māori o Ngai Tahu, University of Otago.
Broughton J. 1995. Te mahi niho hauora ki Ratana Pa: The dental health project at Ratana Pa. New
Zealand Dental Journal 91: 94
–6.
DCNZ – see Dental Council of New Zealand.
Dental Council of New Zealand. 2008. Consultation Document – Draft scope of practice in oral health therapy practice . Released 5 September 2008. Wellington: Dental Council of New Zealand.
Dental Therapy Technical Advisory Group. 2004. Recruitment and Practice of Dental Therapists.
Wellington: Ministry of Health.
DHBNZ
– see District Health Boards of New Zealand.
District Health Boards of New Zealand. 2003. DHB/DHBNZ Workforce Action Plan. Wellington: Ministry of Health.
District Health Boards of New Zealand. 2004. DHBNZ National School Dental Service Review. Final report, December 2004. Wellington: Ministry of Health.
DTTAG
– see Dental Therapy Technical Advisory Group.
Health Workforce Advisory Committee. 2002. The New Zealand Health Workforce Framing Future
Directions Discussion Document . Wellington: Health Workforce Advisory Committee.
Health Workforce Advisory Committee. 2003. The New Zealand Health Workforce: Framing future directions: Analysis of submissions and draft recommendations to the Minister of Health for health workforce development. Wellington: Health Workforce Advisory Committee.
Health Workforce Advisory Committee. 2006. Report of the Health Workforce Advisory Committee on
E ncouraging Māori to Work in the Health Professions
. Wellington: Health Workforce Advisory
Committee.
Health Workforce Information Program. 2009. Workforce Forecast Dental Therapists. Executive summary . Report prepared for The Allied Health Workforce Strategy Group by The Health
Workforce Information Program. Wellington: DHBNZ.
Hollis T. 2000. How accessible is tertiary education to Māori – Part 2. Address given to the National
Forum on Education, University of Canterbury, 17 November 1999 (downloaded 9 August 2005 from http://www.nzine.co.nz/features/Māori_education_2.html?Rcat=Culture&Tcat=Education).
HWAC – see Health Workforce Advisory Committee.
Jefferies R. 1997. M āori Participation in Tertiary Education: Barriers and strategies to overcome them.
Wellington: Te Puni Kōkiri.
Key J. 2008. Speech from the Throne . Delivered by Governor General the Honourable Anand
Satyanand PCNZM, QSM, to Members of the House of Representatives in Parliament
’s Legislative
Council Chamber at the state opening of Parliament (accessed 2 February 2009 at www.beehive.govt.nz).
30
Future Directions for a Māori Dental Therapy Workforce
Koopu P, Keefe-Ormsby V. 2007. Oral health – oranga niho. In Robson B, Harris R (eds) Hauora: Māori
Standards of Health IV . Wellington: Te Rōpū Rangahau Hauora a Eru Pōmare.
Mauri Ora Associates. 2004.
Review of Māori Child Oral Health Services
. Wellington: Ministry of Health.
Ministry of Education. 2005.
Ngā haeata mātauranga: Annual report on Māori education 2004
.
Wellington: Ministry of Education.
Ministry of Education. 2008. State of Education in New Zealand 2008 . Wellington: Ministry of Education.
Ministry of Education. 2009a. Ngā haeata mātauranga – The annual report on Māori education, 2007/08 .
Wellington: Ministry of Education.
Ministry of Education. 2009b. Participation Rates in Tertiary Education . Wellington: Ministry of Education.
Ministry of Health. 2006a. Good Oral Health for All, for Life: The strategic vision for oral health in New
Zealand . Wellington: Ministry of Health.
Ministry of Health. 2006b. Raranga Tupuake.
Māori Health Workforce Development Plan
. Wellington:
Ministry of Health.
Ministry of Health. 2008a. Early Childhood Oral Health: A toolkit for District Health Boards, primary health care and public health providers and for oral health services relating to infant and preschool oral health. Wellington: Ministry of Health.
Ministry of Health. 2008b. Our Future, Our Teeth, A Dentist Workforce Analysis . Wellington: Ministry of
Health.
Ministry of Health and District Health Boards New Zealand Workforce Group. 2007. A Career Framework for the Health Workforce of New Zealand . Wellington: Ministry of Health and District Health
Boards New Zealand.
National Coordination Centre and Regional Coordination Hubs. 2009. Kia Ora Hauora – Māori Health
Careers Programme. National and regional action plan 2008
–2012
. Wellington: National
Coordination Centre and Regional Coordination Hubs.
New Zealand Dental Therapists Association. 2007. Submission to the Ministry of Health on the Review of the Health Practitioners Competence Assurance Act 2003. 5 December 2007. Auckland: NZDTA.
Noonan AS, Evans CA. 2003. The need for diversity in the health professions. Journal of Dental
Education 67: 1030 –3.
Orr J. 1992. Assessing individual and family health needs. In Luker K, Orr J (eds) Health Visiting:
Towards community health nursing (2nd edition). London: Blackwell Science.
Pipi K, Cram F, Hawke R, et al. 2003. M āori and Iwi Provider Success: A research report of interviews with successful iwi and M āori providers and government agencies.
Wellington: Te Puni Kokiri.
Ratima M, Brown R, Garrett N, et al. 2007. Rauringa Raupa: Recruitment and retention of M ā ori in the health and disability workforce . Auckland: AUT.
Ratima M, Waetford C, MacDonald K, et al. 2007. Review of the Ministry of Health Hauora M āori
Scholarship Programme . Auckland: AUT.
Statistics New Zealand. 2010. National ethnic population projections, 2006-base to 2026 update.
Wellington: Statistics New Zealand (accessed 21 October 2010 from the Statistic New Zealand website: www.stats.govt.nz/tools_and_services/tools/TableBuilder/population-projections-tables.aspx).
Tasmanian Department of Health and Human Services. 2003. Allied Health Professional Workforce
Planning Project: Dental therapy information. Hobart: Tasmanian Department of Health and
Human Services, Agency Health Professional Reference Group.
Theobald A, Wong B, Quick A, et al. 2006. The impact of the popular media on cosmetic dentistry. New
Zealand Dental Journal 101: 58
–63.
Thomson WM. 2007. Dental Council of New Zealand – 2006 workforce analysis . Dunedin: University of
Otago.
University of Otago. 2009. Tū Kahika Programme. About Tū Kahika (accessed 6 December 2009 at http://healthsci.otago.ac.nz/tukahika/index.html).
Veal K, Perry M, Stavisky J, et al. 2004. The pathway to dentistry for minority students: from their perspective. Journal of Dental Education 68(9): 938
–46.
Future Directions for a Māori Dental Therapy Workforce
31
Appendix A: Method
The present project set out to take a very broad view of workforce development, looking at what the current Māori dental therapist workforce was and what it might look like in 2018. Future directions for the Māori dental therapy workforce were examined with four scenarios in mind:
1. The alignment of the ethnicity of the workforce with the population it primarily served to see what impact the changing Māori 0–17-year-old population might potentially have on the demand for Māori dental therapists.
2. Examining what optimal ora l health care would be for Māori 0–17-year-olds and what impact this might have on the demand for Māori dental therapists as contributors to oral health service provision.
3. Examining the additional demand for Māori dental therapists if optimal oral health care for Māori 0–17-year-olds was provided by Māori dental therapists, when whānau made this choice.
4. The status quo – namely, what the Māori oral health workforce might look like in
2018 if it was aligned with current institutional provision of Māori dental therapists.
An Australian dental labour force model (AIHW Dental Statistics and Research Unit, 1998;
Australian Health Minister ’s Advisory Council, 2001) was used to examine the oral health service requirements of Māori 0–17-year-olds. This model explored the various pushes and pulls on what could be considered optimal oral health care for this age group.
The Māori health and disability workforce development pathway from Rauringa raupa (Ratima,
Brown et al, 2007) highlighted the need to consider t he role of education in a discussion of Māori dental therapist workforce development. As a result the participation in, and attainment of, secondary school NCEA-level science was examined. Rauringa raupa also emphasised both the role of tertiary education and the transition of graduates into the workforce.
In addition the current project examined local research on, and strategy about, oral health, dental therapy, workforce development and Māori workforce development. Some international research on dental therapy was also included.
When an early draft of the current report had been completed a number of key informants involved in Māori oral health were spoken to. Discussions with key informants largely took place over the telephone, with the interviewer and key informant working through a PowerPoint presentation of the draft report. These discussions were audio-recorded, with key points being transcribed following the interviews. The information supplied by key informants contributed to the revision of the report.
The key informants were:
Associate Professor John Broughton, Department of Preventative and Social Medicine,
University of Otago
Dr Susan Cartwright, Head of Discipline, Oral Health School of Public Health and
Psychosocial Studies, AUT
Vicki Kershaw, Dental Therapist, Immediate past president, Te Ao Marama, Taranaki
District Health Board
Dr Pauline Koopu, Dentist, President, Te Ao Marama
Dr Alison Meldrum, Senior Lecturer, Convenor of Bachelor of Oral Health programme,
Oral Sciences, Discipline of Paediatric Dentistry, University of Otago
Ngaire Mune, Executive Officer, Dental Therapists Association
Kim Smith, Ministry of Social Development
32
Future Directions for a Māori Dental Therapy Workforce
Helen Tane, Senior Lecturer and Oral Health Programme Leader, AUT
Lynette Wilkie, President, Dental Therapists Association
Subsequent drafts of the present report were reviewed by Ministry of Health staff.
Data
The data in the present report was obtained from a number of sources.
The population projections were obtained from the Statistics New Zealand website, using their Table Builder facility (http://stats.govt.nz/methods_and_services/
TableBuilder.aspx). The 2006-base to 2061 projections, Series 6, were used.
Statistics New Zealand now note that this data has been superceded by the 2009-base national population projections (which were not available at the time this report was being written).
The data on the severity of dental caries for 5-year-olds and year 8 children (2002 –
2009) was obtained from the Ministry of Health website (www.moh.govt.nz/moh.nsf/ indexmh/oralhealth-statistics/#adolescent). Projections for 2013 and 2018 were then obtained using the Forecasting function in Microsoft Excel. The R 2 values were also calculated and ranged from 0.00 to 0.76 (with five of the eight values being greater than 0.42).
Predictions for the Māori participation and attainment rates in NCEA science were calculated in the same way as the predictions of severity of dental caries, using
Ministry of Education data that had been analysed by the Ministry of Health
(www.maorihealth.govt.nz/moh.nsf/indexma/science). The R 2 values were also calculated and ranged from 0.01 to 0.98 (with eight of the 12 values being greater than
0.66).
Advice about the productivity of Māori dental therapists (or dental therapists providing optimal oral heal th care to Māori 0–17-year-olds) was provided by Māori oral health providers. A weighting of 50 percent was applied to Māori 13–17-year-olds in the calculation of the caseloads and number of dental therapists required at each productivity level, for both 2006 and 2018 populations (see Appendix C for more information).
Dr Murray Thomson supplied dental therapy workforce data that enabled the examination of the Māori dental therapy workforce in more detail.
Data on the recruitment and retention of Māori students within dental therapy programmes at AUT and Otago were supplied by these institutions.
Future Directions for a Māori Dental Therapy Workforce
33
Appendix B: Supply of dental therapists
In his 2006 DCNZ workforce analysis (the first of its kind for dental therapists) Thomson (2007) reported that there were 683 dental therapists on the Register, 650 (95.2%) of whom held a current APC (although of these 22 were not practising as dental therapists at that time).
29 The majority (72.3%, N = 470) of the dental therapists were in full-time practice. The number of hours worked by the dental therapists (in full- or part-time work) ranged from three to 76, with a mean of 30.7 hours (sd = 12.1 hours).
Thomson analysed the data on these 650 individuals and noted that:
Therapists ’ ages ranged from 21 to 67 with a mean age of 47.9 years (sd 9.8) and a median of 50 years.
Over half of the active dental therapists are aged 50 or more, with 43.4% in the
50 –59 age band. Therapists younger than 40 comprise only one in five of those currently practising.
There are nine male therapists (1.4%), of whom three are in the 20 –29 age group, three are in the 30 –39 age group, and there is one in [each of] the 40–44,
45 –49 and 50–54 age groups (Thomson, 2007, p.46).
The characteristic of the dental therapy workforce that is usually quite strongly highlighted is the average age of the current workforce and the prediction of a decline in the workforce in the next
10 –15 years because of retirements. Ayers et al (2007) reports that more than half of the New
Zealand dental therapists responding to their survey said they planned to retire within 10 years.
The issue is the lack of a replacement pool of dental therapists for these retirees. The SDS and the training of dental therapists were run-down in the 1990s and the current older cohort ‘blip’ is linked to this (cf. DTTAG, 2004).
Historically our problem with the ageing workforce was a lack of training… this has been rectified in recent times with the AUT course, three-year degree course opening up in the last three to four years, but prior to that we only had training in Otago for quite a few years, so that was the limitation for the rest of the country and the numbers taken into Otago training were quite slim
(Informant 3).
One prediction is that if the AUT and Otago programmes each accept 25 dental therapy student first-year admissions each year, it is likely that around 30 (i.e. 60%) of these will enter the New
Zealand workforce upon graduation (DTTAG, 2004). In 2008 there were 23 graduates from
AUT and a similar number is anticipated in 2009 (Informant 4; Informant 3 talked of
28 graduates); in 2009 Otago will graduate its first cohort of 30 students (Informant 10).
Both programmes have increased the number of first-year students they accept. Otago accepted 34 students (with capacity for up to 50) and AUT 36 in 2007. In 2009 AUT accepted
40 first-year students and Otago accepted 41 (Informant 3), so the numbers predicted to enter the New Zealand workforce will rise due to increasing first-year intakes. The question when assessing trends in graduate numbers is whether the new graduates add to the number of dental therapists in the country or merely replace the loss of existing dental therapists (through migration, retirement, alternative careers or death). If it is assumed that by 2018 those who were 50 years of age or older in Thomson ’s (2007) 2006 data will have retired, then the number of retirees from the 2006 workforce will be 334 (51.2%), or over half the workforce.
If 60 percent of graduates enter the workforce each year, in 2008 it can be assumed that
14 entered from the AUT programme. In 2009 32 will enter the workforce from both programmes; and then from 2011 onwards, 48 oral health therapists (60% of the 80 graduates) will enter the workforce each year (i.e. from first-year intakes of 40 to each course beginning in
2009). At this rate the retirees will be well and truly replaced and the workforce increased by
138 dental therapists in 2018 (Table 7).
34
Future Directions for a Māori Dental Therapy Workforce
Table 7: Estimated gain (+) and loss (
–) of dental therapists from the workforce,
2006 –2018
Estimated loss from workforce retirements 2006 to 2018 – 334
+ 510
Estimated gain from graduates of AUT and Otago
(assuming 60% of graduates enter the workforce)
2008 (AUT only)
2009
2011
–2010 (32 pa)
–2018 (48 pa)
+14
+64
+384
Estimated net loss or gain +138
The Health Workforce Information Program (2009) has forecast the workforce demands for dental therapists. (This forecasting does not consider ethnicity.) Of five scenarios the best-case scenario is the addition of 38 dental therapists per annum and the loss of 15 per annum. Their worse case scenario is 23 dental therapists added with a loss of 25 per annum. Their forecasting results were that:
There will not be enough dental therapists for fully expanded service coverage to the
13 –17 year age group.
Partial service expansion to the 13 –17 year age group will lead to a modest oversupply of dental therapists when productivity is modelled at 10.9 visits per day.
The stability of the workforce is more sensitive to departures than to new recruits, with
30 new recruits per year balancing between 20 and 25 departures.
If dental therapists leave the workforce at a rate of 25 per year then an undersupply of dental therapists is almost certain, even with 38 additional therapists joining the workforce per annum.
The five scenarios used in this forecasting appear to be based on the DTTAG (2004) graduate prediction of around 30 new graduates entering the workforce each year, rather than the more up-to-date first-year enrolment and graduation data from AUT and Otago. In addition, the retirement rate of between 15 and 25 dental therapists per annum does not account for the predicted retirement of over half of the workforce by 2018 (Ayers et al, 2007). This is an average rate of approximately 25 per annum all by itself.
Future Directions for a Māori Dental Therapy Workforce
35
Appendix C: Including productivity in the Māori workforce supply calculations
The Health Workforce Information Program (2009) used three dental therapy productivity rates in its workforce forecasts: 10.9, 12 and 15 visits (or appointments) per day. Further examination of the supply of M āori dental therapists in the present report with respect to productivity rates took into account:
advice from M āori oral health providers that, in their experience, 40% of Māori children and young people need to be seen every 12 months, 35% every six months, and 25% need to be seen more regularly (here interpreted as every three months) because of their presenting oral health status 30
d emand for oral care for Māori young people being partially provided by dental therapists (here interpreted as 50% of rangatahi).
When the young person weighting of 50% was introduced into the calculations a slight inequity was introduced between a general population dental therapy service and a M āori population service due to the younger age structure of the M āori population. That is, the number of dental therapists per 100,000 population increased to 68.2 for the general population but to only
67.2 for the M āori population. The application of weightings for both points above produced a required productivity of 13 visits per day for M āori dental therapists, based on 149 Māori dental therapists serving the M āori tamariki and rangatahi population (and using Thomson’s (2007) data that dental therapists, on average, work 30.7 hours per week).
31
Consultation with M āori oral health providers about this productivity rate suggested that it may be too high, with providers reporting that their therapists worked a 7.5 hour day and saw at least
10 tamariki/rangatahi per day. Taking the productivity rate of 10.9 visits per day saw the number of M āori dental therapists needed in 2006 rise from 149 to 178. Even then, the caseload of each dental therapist would be 1246 children and this was considered high by some providers and informants. They suggested that a more appropriate caseload ranged from 700 –1000 children, with the 1000 client caseload requiring 222 M āori dental therapists for Scenario 1 in 2006 (see
Table 8).
Table 8: Productivity, caseload and the number of M āori dental therapists required in 2006, and projected workforce requirements for 2018:
Scenario 1
Productivity 1
8.75
10.9
12
13
15
Caseload
1000.0
1245
1371
1487
1714
Number of Māori dental therapists
2006 2018
222
178
162
149
129
259
208
189
174
151
Note : 1. Productivity is the average number of appointments per day, based on a 30.7 hour week. This is based on 35% of children being seen every six months, 25% being seen every three months and the remainder of the caseload being seen every 12 months.
36
Future Directions for a Māori Dental Therapy Workforce
As can be seen from these calculations, the initial figure of 149 M āori dental therapists needed in 2006 may well be conservative given the experiences of M āori providers of the needs of Māori tamariki and rangatahi and the consequent caseloads that each dental therapist can carry. It should also be noted that the suggestion that some children being seen more than every six months was described by one M āori provider as impractical as ‘there are not enough resources for this to happen ’.
These productivity cal culations were also applied to the projected 2018 Māori 0–17-year-old population. The number of Māori dental therapists ranges from 174 when average productivity is 13 to 208 when average productivity is 10.9. A productivity level of 8.75 was seen as probably unnecessary given that the oral health of this population is predicted to improve. However a productivity level of 15 was seen as probably unattainable given the modest nature of the predicted oral health improvements.
Future Directions for a Māori Dental Therapy Workforce
37
Endnotes
1 ‘It is important to note that the ethnic populations discussed here are not mutually exclusive because people can and do ide ntify with more than one ethnicity’. In addition ‘only series 6 of the respective ethnic population projections [as used in Table 1] and series 5 of the national population projections
[as used here] are designed to be directly comparable’ (Statistics New Zealand, 2010).
2 The establishment of the SDS was premised on a view that children just needed basic oral health care. The social determinants of health, for example, were not considered; thus, the service was set up to fail those at high risk of poor o ral health, especially Māori communities (Informant 4). It should therefore not be surprising that the delivery of oral health services through this mechanism has not led to improvements in the oral health status of Māori children and young people (DHBNZ, 2004).
3 The reason for excluding the 2002 data is that the jump in severity of dental caries between 2002 and
2003 is not sustained in the following years. This appears to make the 2002 data an outlier and may justify its exclusion from the projection calculations. As might be expected, the R 2 value drops with the exclusion of 2002 as a data point (from a range of 0.30
–0.41 to .01–.26), simply because the predictions are then based on less data.
4 There are other recorded counts of the number of Māori dental therapists. The head count of Māori dental therapists in Ministry of Health and DHBNZ (2007) is 48. The Service Specification for this project puts the number of Māori dental therapists at 63, or 4.4% of the dental therapy workforce. An informant also raised the issue of classification of ethnicity
– as in, who says these dental therapists are Māori (Informant 3). The Thomson (2007) data used in the present report was based on selfidentification. Another informant talked about his impression that there were a lot more dental therapists than have been documented based on the number of Māori dental therapists attending the
Te Ao Marama hui, 80
–100 perhaps (Informant 5). Not all these Māori dental therapists may hold current APCs and/or be identifi ed as Māori in the DCNZ database.
5 There is no guidance on a recommended ratio of dental therapists per 100,000 0
–17-year-olds in the population. A 2002 Tasmanian report raises this issue but as every Australian state has its own practising regulations it is difficult to come up with one standard ratio (Tasmanian Department of
Health and Human Services, 2003). There is mention of 70 oral health professionals per 100,000 population in New Zealand, but this encompasses all professionals, including dentists (Ministry of
Health, 2008).
6 This may be because they have tried to and not had a good experience, or they may not see this as a career choice. For whatever reason, the choice that Māori dental therapists have about whether or not to work with Māori has to be acknowledged. There is a range of factors that impact on workplace decisions for all dental therapists, and this is also the case for Māori dental therapists. This includes location, remuneration, practice orientation, preference to work for Māori or non-Māori organisations and/or with Māori or non-Māori tamariki and rangatahi. It may also be that Māori dental therapists, with experience of working with Māori and other minority groups, will be recruited to jobs overseas by countries committed to addressing oral health disparities.
7 At present it is not known what proportion of the those graduating as oral health therapists will work as dental therapists and what proportion will work as dental hygienists. Many of the AUT graduates in
2008 got jobs with the DHB as dental therapists. Only a few went into private practice (Informant 7).
This is not to say that dental hygienists are not an important part of oral health care for Māori (but this report does not consider this need).
8 Participation rate is calculated from the number of students doing at least one credit in a science subject, as a percentage of the total number of candidates across all subjects in that year group
(Ministry of Health website, www.maorihealth.govt.nz/moh.nsf/indexma/science-nationalparticipation).
9 The 2004 –2009 data (percentage participation) has been used to predict Māori and non-Māori participation rates in 2013 and 2018. An alternative predication method would be to use predicted absolute numbers of students and then describe this as a percentage of the age group population. As this makes assumptions about the participation of young people in school that may be inaccurate, the predictions here are based on the percentage data from the Ministry of Health participation tables
(www.maorihealth.govt.nz/moh.nsf/indexma/science-nationalparticipation).
38
Future Directions for a Māori Dental Therapy Workforce
10 A student is counted as having attained science if they have achieved 14 or more credits in a science subject. Attainment rate is calculated as the number of candidates to gain 14 or more credits, as a percentage of the number of candidates participating in the subject at that year level
(www.maorihealth.govt.nz/moh.nsf/indexma/science-nationalattainment).
11 The 2004 –2009 data (percentage attainment) has been used to predict Māori and non-Māori participation rates in 2013 and 2018.
12 A New Zealand Council of Educational Research (2006, p.vi) study of students in science found that:
The same types of factors appear to impact on individual students’ decisions about continuing with science at both secondary and at tertiary levels, with some changes in the sources of advice students might access as they transition to tertiary studies.
Students’ choices relate to their personal interests and decision-making orientations, their family background, their learning experiences
– both curricular and extracurricular
– and the school they attend.
While there were low numbers of Māori students in its survey sample, the study noted that nationally there were low levels of participation in science by students at low decile schools. Their conclusion was that more research needed to be done as low participation rates by Māori students in science could be related to low participation rates more generally at low decile schools.
13 However, as an informant described it, oral health was considered the ‘non-sexy’ health career option when compared with medicine. Research in the United States found that minority applicants to dental schools mostly found out about dental training programmes from a friend or family member rather than from any intentional recruiting effort, and that hearing from a minority student already in the programme was pivotal to their decision-making (Veal et al, 2004).
14 Māori secondary school students have highlighted their need for role models who can talk with them about health-related career options (Ratima, Brown et al, 2007a). However, an informant described how, apart from the Kura Kaupapa Māori, no secondary schools in her area were interested in having oral health professionals talk with their students (Informant 1).
15 Auckland University of Technology (2007a, p.180) recommends ‘... quality course and career information, [and] advice and counselling to support the transition from secondary school to tertiary study’. The Mauri Ora (2004, p.33) review of Māori child oral health services also recommends that:
Māori providers should be encouraged to develop their own oral health workforce through their relationships with training establishments and the development of further treatment services where Māori can gain important community experience and attraction to the oral health professions.
DHBs can also provide this type of practical experience for Māori thinking of a career in dental therapy.
16 The DHBNZ (2004) review noted that salary packages for dental therapists were unattractive and that this was an ‘obvious workforce issue’ (p.20). This is changing in response to DHBNZ’s call for a
‘national review of dental therapy salary and conditions of employment’ (also see DTTAG, 2004).
Currently there has been upward salary movement with a new oral health therapy graduate being paid around $35,000 per annum (Informant 10). Government moves to address chronic workforce shortages may also see students studying dental therapy being eligible for student loan write-offs
(Key, 2008), and this may also increase the incentive for students to enter oral health therapy programmes.
17 Older dental therapists are more likely to have a Certificate in Dental Therapy or a Diploma in Dental
Therapy. Certificate and Diploma courses are no longer offered by a tertiary institution in this country.
Other qualifications that dental therapists might have include:
an undergraduate dental therapy degree or diploma from an Australian Dental Council accredited educational programme
an undergraduate dental therapy degree or diploma, or an undergraduate dental degree, and a pass in the DCNZ Dental Therapy Registration Examination
a Graduate Diploma in Dental Therapy (Otago).
Some overseas-trained dentists have passed the Dental Therapy Registration Examination so that they can practice as dental therapists in this country (Informant 10).
Future Directions for a Māori Dental Therapy Workforce
39
18 Historically, the Māori participation rate in tertiary health education programmes has been low compared to the nonMāori rate (Ministry of Education, 2005). Between 2001 and 2004 there were
22 Māori students enrolled in dental hygiene and therapy courses. During the 2001–2003 period, seven Māori completed dental hygiene or dental therapy courses (Ratima, Brown et al, 2007).
19 Up until the HPCA Act 2003 dental therapists practiced under the supervision of a dentist
(Informant 6). Dental therapists are able to practice independently within their scope of practice, without the physical presence of a den tist. They must have a ‘consultative working relationship’ with a dentist in order to get their practising certificate (DCNZ, 2008, p.6). This is a signed agreement between the two parties under which the dentist audits the dental therapist’s clinical work and treatment planning (Informant 10). DCNZ has recommended that this arrangement continue for the oral health therapists created by the new AUT and Otago oral health degrees.
20 There are 15 dental therapists currently trained for dental therapy scopes on adults (Thomson, 2007) and more might take up this opportunity if the training were available in this country, which it is not.
The current barriers, identified by an informant, to the provision of adult scope training at Otago are:
a perceived low level of interest among staff at Otago
high course costs
an unwillingness of dental therapists to pay for the course or to go to Otago to do it
(Informant 10).
On the other hand, AUT developed an adult scope course but was not accredited by the DCNZ to provide it (Informant 4). NZDTA (2007) notes that since the HPCA Act 2003 came into force in 2004 only two people with overseas experience have registered in the adult scope.
21 In anticipation of these new graduates the Dental Council of New Zealand (DCNZ) produced a consultation document on a draft scope of practice in Oral Health Therapy Practice in September
2008, with submissions due 17 October 2008. The new scope of practice combines the General
Dental Therapy and General Dental Hygienist scopes (which will also remain as separate scopes for practitioners wishing to register in one scope), reflecting the ‘full range of tasks that graduates are able to undertake’ (DCNZ, 2008, p.3). This was still a draft scope at the time the present report was written.
22 New graduates may also need to ‘keep their heads down’ when they are out in the school dental clinics because their more recent training means they know more about oral health care than their older professional counterparts. This has been redressed somewhat since 2003 by the training that
DHBs have been providing for the latter group (Informant 4).
23 The Ministry of Health and DHBNZ (2007, p.5
–6) acknowledged the need for healthy and sustainable workplaces so that staff can be recruited and retained.
To support the recruitment and retention of staff, the health sector must be a safe, supportive and productive environment. The main elements of healthy workplaces include conditions of employment for health workers, the physical work environment, equal opportunity, cultural diversity, wellness practices, and relationships with the wider social environment.
24 Regional variation in working conditions is also an issue and may have an impact on where dental therapists choose to work. Starting salaries for graduates, for example, can vary between $35,000 and $42,000 per annum (Informant 4). ‘There is huge variation in some areas where some [dental therapists] get 12 weeks
’ annual leave, based on the school year, and other DHBs only give six weeks’
(Informant 3).
‘The [School Dental] Service has changed since DHBs started running their own shows; there is no consistent approach in New Zealand any more’ (Informant 7).
25 These positions tend to be for people who are good dental therapists rather than for dental therapists who have gained a good understanding of public health or managerial skills (Informant 6).
26 DHBNZ (2004, p.7) recommended postgraduate study as a general way to ‘up skill and extend dental practice’. However, there also needs to be career rewards for this.
40
Future Directions for a Māori Dental Therapy Workforce
27 Validation of these ‘Māori preferred-employer criteria’ (although not specifically referred to) can be found in the recent research finding that Māori workforce retention depends on institutional commitment to Māori workforce development (Ratima, Brown et al, 2007, p.xvii). This includes:
... a culturally safe work environment; recognition and valuing of Māori cultural competencies and practice models; access to clinical supervision and Māori resources; paid professional development opportunities to gain and strengthen cultural competencies; opportunities to work in Māori settings and to use Māori practice models in Māori contexts; culturally safe management.
28 The monitoring of whether their work environment is supportive of Māori dental therapists in this way may require the development of an organisational audit tool. This will only be useful if and when there is organisational commitment to reviewing and strengthening the support provided for Māori staff.
29 Other counts of the dental therapy workforce have been undertaken. DTTAG (2004) reported that in
2003 there were 508 full-time equivalent (FTE) dental therapists employed by the DHBs (with
24 vacancies). DHBNZ (2007) counted 991 dental therapists, or 786.4 FTEs. Thomson (2007) is used in the present report as it is the first detailed analysis based on APCs. Data from 2007 was available but not as a detailed breakdown, resulting in a decision to use the 2006 analysis (Thomson,
2007).
30 Dental therapists only see children once every 12 mont hs but it is anticipated that the Māori need for oral health services will be great because of the state of their oral health, and also the need to change behaviour and put prevention in (e.g. fluoride applications) (Informant 10). They will therefore need to be seen every six months (Informant 3), and earlier – at 6–9 months (Informant 10). DHBNZ (2007) recommended that recall periods for low-risk children be revised in order to treat those in need. This may be difficult for Māori dental therapists treating Māori children who find that a large proportion of their client base is high need.
31 Key informants did note that DHBs are now more likely to require dental therapists to work a full
37.5 hour week.
Future Directions for a Māori Dental Therapy Workforce