Calf Venous Compliance in Endurance Trained Females
advertisement

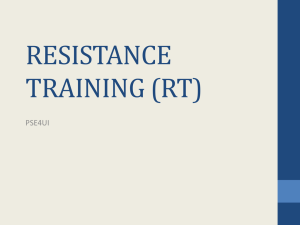
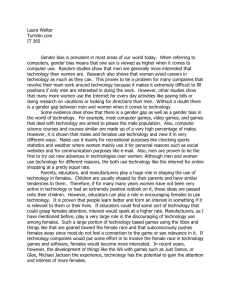
Venous Compliance in Trained Females 39 Journal of Exercise Physiologyonline (JEPonline) Volume 12 Number 4 August 2009 Managing Editor Tommy Boone, PhD, MPH Editor-in-Chief Jon K. Linderman, PhD Review Board Todd Astorino, PhD Julien Baker, PhD Tommy Boone, PhD Larry Birnbaum, PhD Eric Goulet, PhD Robert Gotshall, PhD M. Knight-Maloney, PhD Len Kravitz, PhD James Laskin, PhD Derek Marks, PhD Cristine Mermier, PhD Chantal Vella, PhD Ben Zhou, PhD Official Research Journal of the American Society of Exercise Physiologists (ASEP) ISSN 1097-975 Sports Physiology Calf Venous Compliance in Endurance Trained Females JULIANE P. HERNANDEZ, BETSY E. GODAR Department of Kinesiology, Southern Illinois University, Carbondale, Illinois ABSTRACT Hernandez, JP, Godar, BE. Calf Venous Compliance in Endurance Trained Females. JEPonline 2009;12(4):39-49. Endurance training has been shown to increase calf venous compliance in males, but the effects of endurance training on calf venous compliance in females have yet to be established. The purpose of this investigation was to determine the effects of endurance training status on the calf venous compliance in young females. Twenty healthy endurance trained collegiate track and cross country athletes [10 female (20.50.4 yrs, 59.41.6 ml*kg-1*min-1) and 10 males (22.91.3 yrs, 64.3 2.8 ml*kg-1*min-1)], and twenty healthy average [10 female (21.70.5 yrs, 35.91.8 ml*kg-1*min-1) and 10 male (23.71.0 yrs, 42.61.8 ml*kg-1*min-1)] volunteers underwent maximal graded exercise tests and assessment of calf venous compliance. Utilizing venous occlusion plethysmography, calf venous compliance was determined in both groups using the first derivative of the pressure-volume relation during cuff pressure reduction. Venous capacitance and capillary filtration volumes were determined following cuff pressure inflation. VO2max was significantly greater in the endurance trained females and males compared to the average-fit females and males (p<0.05). The endurance trained females had higher calf venous compliance than the average fit females (p<0.05; ~40%; 0.0022 vs 0.0013 ml 100ml-1 mmHg-1), and the endurance trained females had significantly greater capillary filtration volumes than both of the average fit groups and the endurance trained males (p<.05). Endurance trained females have greater calf venous compliance than females of average fitness. Key Words: Peripheral Circulation, Training, Gender, Blood Flow. Venous Compliance in Trained Females 40 INTRODUCTION The venous vasculature is a volume reservoir containing approximately 70% of our total blood volume. This system is designed to preserve flow of blood from the tissues to the heart during cardiovascular stress. Variations in blood volume can be overcome by altering the total capacity of the venous system to maintain pressure, thus ensuring venous return to the heart (1,2). This pressure-volume relationship is an important part of cardiovascular homeostasis. Veins are 30-50 times more compliant than arteries and in the upright posture 70% of the blood volume falls below the level of the heart. This translocation of blood away from the heart causes a stress to the cardiovascular system that is counter-regulated by sympathetic modulation, specifically higher peripheral resistance and increases in heart rate as well as activation of the skeletal muscle pump (2, 3). Endurance trained male athletes have consistently higher venous compliance in the calf than their more sedentary peers (4,5). However, this training affect has not been directly assessed in females and recent research suggests that calf venous compliance in untrained females is lower than that of untrained males (6,7). Females are more prone to orthostatic intolerance than males (8,9, 10, 11) and female runners appear to be more susceptible to hypovolemic intolerance than non runners (12). Therefore the primary purpose of this investigation was to determine the calf venous compliance in endurance trained females compared to their counterparts of average fitness. We hypothesized that calf venous compliance would be significantly higher in the endurance trained than in the normally active females. METHODS Participants Twenty healthy endurance-trained track and cross-country athletes (10 female and 10 male) were recruited from a Division I University along with twenty (10 female and 10 male) volunteers of average fitness from the university. The endurance trained athletes were matched as closely as possible for training volume and VO2max. The average fit participants reported no regular physical activity defined as exercising 20-45 minutes 3 times per week. All participants were healthy based on medical history, resting blood pressure < 140/90 mmHg, no reported use of tobacco, body fat percentage < 35%, free of any diagnosed cardiovascular disease and not taking any cardiovascular medication. There was no known venous insufficiency and participants refrained from caffeine ingestion for 12 hours and food consumption for 1 hour before testing. Data collection was performed at a stable room temperature between 23-25°C. Female participants were tested in the follicular phase (3-10 days from the first day of menstruation) of their menstrual cycle, and all reported regular menstrual cycles. Written informed consent was obtained according to practices established by the Southern Illinois University Human Subjects Committee. Experimental Procedures A balance scale and stadiometer were used to assess body mass (kg) and height (cm). Body composition was estimated by a 3-site protocol using Lange Skinfold Calipers. Maximal oxygen consumption was measured during graded treadmill exercise to exhaustion using open-circuit spirometry (TrueMax 2400 ParvoMedics). Standard criteria for achievement of valid maximum oxygen consumption was met in all participants (13). Strain gauge plethysmography (ECR5 Hokanson, Bellevue, WA) was used to assess changes in calf volume and a venous collecting cuff was used to control pressure (AG101 Hokanson, Bellvue, WA). Blood pressure and heart rate were continuously monitored by Dinamap (J & J Medical, Tampa, FL) non-invasive blood pressure monitor. Venous Compliance in Trained Females 41 Experimental Protocol The methods selected for the present study were similar to those used previously by Hernandez and Franke (2004), a slightly modified version of the procedures validated by Halliwill et al. (1999). Participants reported to the laboratory on two separate occasions. The first visit was to obtain anthropometric data and perform a VO2 max test to determine fitness level. Using the formula r2L, calf volume was calculated from four girth measures obtained equidistantly between the medial malleolus and the tibial plateau and one calf segment length. Venous compliance measurements were conducted on the second visit, which was at least 48 hours after the treadmill test. Changes in calf volume were assessed non-invasively using strain gauge plethysomography. With the participant in a supine position the right leg was elevated above heart level and supported at the ankle and thigh to promote venous drainage. A venous collecting cuff was applied proximal to the right knee and connected to an external air source that allowed pressure to be precisely and rapidly modulated within the cuff. A mercury in-silastic strain gauge was placed around the maximal circumference of the calf. After instrumentation and 30 minutes rest, venous collecting cuff pressure was applied at 60 mmHg for 8 minutes and subsequently reduced by 5mmHg /5s to 10 mmHg. At the onset of cuff pressure, an initial rapid increase in the volume of the calf occurred which is associated with the capacitance response (16) followed by a slower, but continuous rise in volume caused by net transcapillary fluid filtration from blood to tissue as described by Schnizer and colleagues (1978, 17). During cuff pressure reduction (5mmHg/5 seconds) volume declined rapidly (Figure 1). Data Analysis All data were recorded on a Dell PC (Biopac data acquisition software) for analysis. Resulting pressure-volume curves during the step down in pressure are described by the quadratic regression equation [( limb volume) = 0 + 1(cuff pressure) + 2(cuff pressure)]. The group-average regression parameters 1 and 2 were used together as an estimate of compliance [compliance = 1 + 22(cuff pressure)]. The first derivative yields a linear pressure-compliance relationship and this slope was used to determine training (endurance vs. average fit) and sex (females vs. males) differences. The capacitance response was calculated from the volume increase at the onset of cuff pressure to the line defined from the filtration slope between 3 and 8 minutes of cuff pressure application. Total capillary filtration during cuff pressure was calculated from the rate of filtration (ml/min) times the time of the cuff pressure application (8 min). Total calf volume increase was the sum of the capacitance and net capillary filtration volumes. Differences in participant characteristics, compliance regression parameters, capacitance, and capillary filtration volumes were determined using two-way ANOVA (fitness X gender). Statistical significance was set at p<.05. When significance was revealed by the ANOVA, group differences were located using the Student Newman-Keuls post hoc test. RESULTS Participant Characteristics Physical characteristics are summarized in Table 1. VO2max was significantly greater in the endurance trained groups compared to the sedentary groups (p<.05). Both average fit groups and the endurance trained males had a greater body mass than the endurance trained females (p<.05). The average fit females had a greater body fat percentage than all other groups and the endurance trained males had a lower body fat percentage than all other groups (p<.05). Body mass index was greater in the average fit groups than the endurance trained groups (p<.05). The average males had higher systolic blood pressure than all the other groups and a higher resting heart rate than the endurance trained males (p<.05). Height was greater in the males of both average and endurance Venous Compliance in Trained Females 42 trained groups than the females (p<.05), and calf volume was significantly lower in the endurance trained Table 1. Selected Participant Characteristics. females than Variables Average Fit Average Fit Endurance Endurance all other Female Male Trained Trained groups Female Male (p<.05). 21.7±1.7 23.7±3.2 20.5±1.4 22.9±3.9 Age (yr) 164.9±6.0bd 174.5±4.7 167±5.2bd 179.2±4.3 Height (cm) c c 75.3±12.5 85.7±16.0 58.6±8.2 72.8±6.6c Body Mass (kg) ac a 29.8±3.6 17.7±5.3 16.5±2.8 12.0±4.8abc Bodyfat (%) 27.6±3.6 28.1±4.6 20.9±2.1ab 22.7±2.0ab BMI acd 122.1±11.6 127.1±11.0 111.5±8.8 117.6±7.3 Systolic BP (mmHg) 85.0±8.8c 89.4±8.4c 70.2±9.4 76.8±6.1b Diastolic BP (mmHg) 76.7±6.8d 67.4±10.5 61.7±6.2 Resting Heart Rate (bpm) 68.0±7.6 3725.1±560 3912.2±523 3106.2±381abd 3608.3±309 Calf volume (ml) VO2max (ml*kg-1*min-1) 35.8±5.6 42.5±5.8 59.4±5.1ab 64.3±9.0ab Values are means SD; n = 40 (10 in each group). VO2max, maximal oxygen consumption; BP, blood pressure; BMI, body mass index. ap< 0.05 vs. average females; bp< 0.05 vs. average males. cp<0.05 vs. endurance trained female. d p<0.05 vs. endurance trained male. Calf Venous Compliance Table 2 displays the regression parameters 0, 1, and 2 calculated (means SD) for average and endurance trained females and males. In both average groups, pressure-volume curves derived from the calf were less steep than in the endurance trained groups (p<.05; Table 2 and Figure 2). The pressure-volume and compliance-pressure curves illustrate these differences in Figures 2 and 3. Calf venous compliance was lower in the average fit groups than the endurance trained participants (Figures 3 & 4). Endurance trained females were ~40% more compliant than average females (p<.05; 0.0022 vs 0.0013 ml 100ml-1 mmHg-1) and endurance trained males had ~50% greater compliance than average males (p<.05; 0.0025 vs 0.0012 ml 100ml-1 mmHg-1; Figures 3 & 4). Calf venous compliance differences were quantified using the slope of the compliance-pressure line. Calf venous compliance between the females and males did not differ significantly in either fitness group (Figure 3 & 4). When training differences were quantified by calculating percent change in β1 at an intravenous pressure of 0 mmHg (5) the endurance trained females were ~35% more compliant than the average females and the endurance trained males were ~ 47% more compliant than the average males (p<.05). Two methods of quantifying compliance were used in order to compare the present findings with previous research (5) that used different methods of quantifying compliance differences. The endurance trained females and males had greater capacitance responses than did the average fit groups (p<.05; Figure Table 2. Pressure-Volume Regression Parameters. β0 β1 β2 5). 0.9559±.4971 0.0797±.0223cd -.0007±.0002cd Average Female Interestingly, 1.1415±.7469 .0751±.0286cd -.0006±.0003cd the endurance Average Male abd 2.3544±1.1253 .1230±.0229 -.0011±.0003 Endurance Trained Female trained Endurance Trained Male 1.3434±.8413 .1428±.0264 -.0012±.0002 females had Values are means + SE. Δ Calf Volume = β0 + β1 *(cuff pressure) + β2 *(cuff significantly pressure)2; ap< 0.05 vs. average females; bp< 0.05 vs. average males. cp<0.05 vs. greater endurance trained female. dp<0.05 vs. endurance trained male. capillary filtration volumes than both of the average groups and the endurance trained males (p<.05; Figure 5). There was no difference between males and females in capacitance volumes in either the average groups or the endurance trained groups. Total calf volume increase was greater in the endurance trained groups than the average fit group (p<.05; Figure 5), but not different between the sexes in either group. Venous Compliance in Trained Females 43 DISCUSSION Chang in Volume (ml/dl) Pressure (mmHg) To the best of our knowledge this is the first study to investigate differences in lower limb venous compliance between endurance trained female athletes and females of average fitness. Based on previous findings in males (4,14), we 60 hypothesized that calf venous compliance would be higher in the endurance trained than in the normally active females. The main findings of the study support this hypothesis showing that endurance trained females have significantly 0 greater venous compliance, capacitance volume, and net capillary filtration volumes than their average fit peers. This is consistent with previous research conducted primarily in males 6 (4,14,18). Interestingly, we did not find a gender difference in calf venous compliance in either the endurance trained or the average fit group. This is in direct contrast to earlier investigations (6, 7). We did however find that the endurance trained 0 females had significantly greater capillary filtration volumes than either of the male groups 0 3 6 9 and the average fit females. Time (min) Figure 1. Original tracing showing calf volume Figure 1.in response to 60 mmHg cuff pressure changes applied to the thigh for 8 minutes and subsequent reduction in pressure of 5 mmHg/5 seconds in a 21 year old endurance trained male. Endurance Training The finding of increased calf venous compliance in endurance trained females compared to their normally active peers supports Monahan and colleagues (2001) and Hernandez and Franke (2005), showing endurance training is associated with higher calf venous compliance in males. Monahan and colleagues (2001) found a significant positive correlation between calf venous compliance and maximal oxygen consumption in a group of sedentary and trained older and young men (r = 0.07). However, in a previous investigation, we did not find as strong a correlation between calf venous compliance and maximal oxygen consumption (r = 0.297) despite significantly higher calf venous compliance in the trained groups. Our previous investigation included females in the groups of older and younger, trained and sedentary individuals, and it was initially speculated that the females may have affected the relationship between fitness and compliance, but when separated for gender, there was inadequate statistical power (5). To the best of our knowledge, this is the first study to show the capacitance and capillary filtration volumes in endurance trained and normally active men and women using the pressure reduction method of non-invasively assessing compliance (17). Total calf volume increase was greater in the endurance trained females than their normally active counterparts (p<.05). The capacitance response of the endurance trained athletes was almost twice as much as the volumes seen in the normally active individuals. The capillary filtration volumes were greater in the female athletes than the female normally active participants while there was no difference in the capillary fitration volume with endurance training in men. The capacitance response in the athletes is most likely being driven by the higher compliance of the vasculature as well as higher blood volumes and greater capillarization (2). Lindenberger and Lanne (2007) found that application of lower body negative pressure (LBNP; 11, 22 & 44 mmHg) yielded increases in capillary filtration volumes with higher Venous Compliance in Trained Females 44 pressures in men and women. Further, they found that the women had higher capillary fitration volumes than the men at the lower LBNP . The fact that our cuff pressure application (60 mmHg) was the same for all groups indicates a possible differential response in the vasculature of females to training. The participants assessed by Lindenberger and Lanne (2007) were described as healthy and of average fitness, but they may have been slightly more fit than the average fit group used in the current investigation. Lindenberger and Lanne (2007) reported a mean resting heart rate of 61 (2) beats per minute and a resting systolic blood pressure of 107(1) mmHg, while the average fit females in the current investigation had a mean resting heart rate of 68(2) beats per minute and a systolic blood pressure of 122 (4) mmHg. The gender difference in the capillary filtration volumes will be discussed in the next section (18). A. B. Compliance (ml/dl/mmHg) Volume (ml/dl) Possible mechanisms for 7 7 alterations in calf venous 6 6 compliance are quite similar to 5 5 those on arterial central 4 4 compliance. Compliance of 3 3 veins appears to decline with age and improve with chronic 2 2 physical activity comparable to 1 1 central arterial compliance (19). 0 0 0 10 20 30 40 50 60 0 10 20 30 40 50 60 Mechanistic speculations on 0.16 0.16 changes in venous compliance 0.14 0.14 Average Female Average Male have focused on alterations in Endurance Endurance Trained 0.12 0.12 Trained Female Male the ratio of elastin to collagen in 0.1 0.1 the vessel wall or changes in 0.08 0.08 the vessel composition caused 0.06 0.06 by alterations in sympathetically 0.04 0.04 meditated vascular quality (6, 7, 0.02 0.02 18). Halliwill et al. (1999) 0 0 0 10 20 30 40 50 60 0 10 20 30 40 50 60 demonstrated sympathetic Pressure (mmHg) Pressure (mmHg) stimulation did not affect Figure Figure 2. 2. Volume-Pressure curves (top) and Volume-Compliance venous compliance, suggesting Slopes (bottom) for A. Average fit and endurance trained females venous vasculature compliance (red) and B. Average fit and endurance trained males (blue). is increased by alterations in Means + SD. The endurance trained groups had significantly the composition of the vessel steeper compliance slopes than the average fit groups (p<.05) as wall. In contrast, Monahan and shown in Table 2. Ray (2004) showed that sympathoexcitation reduced venous compliance, but only in men. Hernandez and Franke (2004) found no changes in calf venous compliance in an older population after 3 months of endurance training, but reported an improvement after 6 months that wasn’t significant but probably meaningful (p = .07), implying alterations may take time to occur supporting the idea of vessel wall remodeling. Further research exploring the mechanisms responsible for increasing venous compliance with endurance training is still warranted. Gender Differences Monahan and Ray (2004) found females to have 48% lower calf venous compliance than males and Meendering et al. (2005) reported a 26% greater compliance in the males than the females. The magnitude of the reported gender differences is likely attributable to the way the compliance differences were quantified and/or the fitness levels of the participants, which weren’t reported in the previous studies. In pursuit of the mechanism responsible for differences in calf venous compliance Venous Compliance in Trained Females 0.16 0.14 Average Female Average Male 0.12 Compliance (ml/dl/mmHg) between men and women, Meendering et al. (2005) measured calf venous compliance during the early follicular, ovulatory, and midluteal phases of the menstrual cycle, and compared these findings to men. Their data showed that females had lower calf venous compliance than males but also suggested that calf venous compliance does not change with menstrual cycle phase (4) and therefore gender differences in venous compliance are probably not related to fluctuating hormone levels. 45 Endurance Trained Female 0.1 Endurance Trained Male 0.08 0.06 0.04 0.02 0 0 10 20 30 Pressure (mmHg) 40 50 60 Figure 3. Figure 3. Compliance-Pressure slopes for average females, average males, endurance trained females, and endurance trained males. Slope of Compliance Recently, Lindenberger and Lanne (2007) assessed sex differences in venous compliance in the lower limb using three different levels of lower body negative pressure (LBNP) as opposed to the cuff pressure application method utilized in the present investigation and others (,5,7,14,18). They found that calf venous compliance was reduced in women compared to men only at low 0 transmural pressures (11 & 22 mmHg) but disappeared at a higher 0.0005 pressure (44 mmHg). Further, they found that capillary fluid filtration was greater in the females than the males 0.001 at the lower distending pressures, probably due to a higher capillary fluid 0.0015 coefficient in the women. The sex differences in compliance were not seen when the contribution of 0.002 capillary filtration was not accounted for (18). The present investigation 0.0025 assessed compliance during pressure reduction at a rate of 5 mmHg/5 Endurance Trained Average Female Average Male Female Endurance Trained Male seconds (Figure 1) which should have 0.003 been fast enough to remove the Figure 4. Slope of the compliance-pressure relationship. potential effects of differences in Means + SD. ap<.05 vs average females; bp<.05 vs average capillary fluid filtration and males characterize volume changes over a large pressure range (10-60 mmHg; 15). If capillary filtration differences between men and women are driving the compliance differences that have been seen previously, then the method utilized in the current investigation should consistently reveal no sex difference in compliance, but that has not been the case. Whether this is due to the methodology or the fact that capillary filtration is not affecting compliance assessment requires further investigation. ab ab Venous Compliance in Trained Females 46 One possible explanation for the discrepancy in our current findings compared to previous research showing that young females have lower venous compliance than males may be that our average fit males and females had a higher body mass and BMI than that reported in previous studies (6,7,18). The average females had a bodyfat percentage of 29.8 versus 17.7 in the average males. Oren et al. (1996) assessed arterial and venous compliance using central blood volume indices and reported that obesity increased central arterial compliance but had no effect on the capacitance of the venous system (21). However, Stepniakowski and Egan (1995) reported reduced venous dispensability in the forearm of obese individuals (22). Neither of these studies assessed venous compliance in the lower limb or across a range of distending pressures. Obesity has been associated with an increased resting muscle 7 sympathetic nerve activity, but as Monahan 6 and Ray (2004) demonstrated, 5 1.5528 sympathoexcitation in 1.2364 females doesn’t appear to alter venous 4 compliance. Therefore, 1.2374 0.8526 if females have less 3 compliant veins than males as suggested 4.2988 4.221 previously (6,7,18), then 2 it’s possible that the 2.8824 2.8136 equivalent compliance 1 found in the present study may be due to the 0 higher body fat of the Endurance Trained Female Endurance Trained Male Average Male Average Female females. The role Capillary Filtration Capacitance obesity plays in alterations of venous Figure 5. Contribution of capacitance response (solid bars; bottom) and compliance deserves capillary filtration response (shaded bars; top) to increases in calf further investigation. To volume with cuff pressure application of 60 mmHg for 8 minutes. Means date, mechanisms + SD. ap< 0.05 vs. average females; bp< 0.05 vs. average males; cp<0.05 associated with gender vs. endurance trained male differences have primarily focused on hormonal contribution (6), responses to baroreceptor unloading (7), and capillary filtration differences (18). Gender differences in the structure of the vessel wall are yet unknown, although estrogen receptors have been found in smooth muscle cells and may affect cellular transcription of elastin and collagen (23,24). Future endeavors may want to match participants on body fat levels as well as the fitness, age and gender of the participants when determining lower limb venous compliance. Calf Volume Increase (ml/dl) abc ab ab Several limitations should be considered when evaluating the results of this investigation. First, in utilizing venous occlusion plethysmography to non-invasively assess venous compliance, the venous collecting cuff pressure is used as a substitute for venous pressure; therefore this is really a measure of whole limb compliance. Secondly, the participants included endurance athletes who participated in sports involving the lower limbs; it is likely any adaptation to endurance exercise may be localized in the trained limbs. Therefore, it is possible that different results may be observed if venous circulation in other areas of the body is studied such as in the pelvic region where women tend to pool more Venous Compliance in Trained Females 47 blood than men (7), or in athletes who train using a predominantly gravity independent environment such as swimming. Lastly, only young healthy adults were investigated in the present study. Therefore, our results cannot be generalized to other age groups or patients with other conditions. CONCLUSIONS In conclusion, endurance trained females have greater calf venous compliance than their more sedentary peers. While previous studies have shown that females have lower calf venous compliance than males (6,7), this investigation found that there was no difference between the sexes in either the highly trained group or the groups of average fitness. More investigation into potential sex differences is necessary to determine what is causing these discrepant findings. Address for correspondence: Juliane P. Hernandez, Ph.D., Department of Kinesiology, 1075 S. Normal, Southern Illinois University, Carbondale, IL 62915-4310. Phone (618)453-3124; FAX: (618)453-3329; Email. juliane@siu.edu. REFERENCES 1. Rothe CF. Physiology of venous return. An unappreciated boost to the heart. Arch Int Med 1986;146:977-982. 2. Rowell LB. Human Cardiovascular Control. New York: Oxford University Press. 1993. 3. Rothe CF. Reflex control of veins and vascular capacitance. Physiol Rev 1983;63:12811342. 4. Monahan KD, Dinenno FA, Seals DR, and Halliwill JR. Smaller age-associated reductions in leg venous compliance in endurance exercise-trained men. Am J Physiol Heart Circ Physiol 2001;281(3):H1267-H1273. 5. Hernandez JP and Franke WD. Effects of a 6-month endurance-training program on venous compliance and maximal lower body negative pressure on older men and women. J Appl Physiol 2005;99(3):1070-1077. 6. Monahan KD and Ray CA. Gender affects calf venous compliance at rest and during baroreceptor unloading in humans. Am J Physiol Heart Circ Physiol 2004;286(3):H598H901. 7. Meendering JR, Torgrimson BN, Houghton BL, Halliwill JR and Minson CT. Effects of menstrual cycle and oral contraceptive use on calf venous compliance. Am J Physiol Heart Circ Physiol 2005;288(1):H103-H110. 8. Convertino, V. Gender differences in autonomic functions associated with blood pressure regulation. Am J Physiol Regul Integr Comp Physiol 1988;275(44):R1909-R1920. 9. Gotshall, R. Gender differences in tolerance to lower body negative pressure. Aviat Space Environ Med 2000;71(11):1104-1110. Venous Compliance in Trained Females 48 10. Shoemaker JK, Hogeman CS, Khan M, Kimmerly DS, and Sinoway L. Gender affects sympathetic and hemodynamic response to postural stress. Am J Physiol Heart Circ Physiol 2001;281:H2028-H2035. 11. White DD, Gotshall RW and Tucker A. Women have lower tolerance to lower body negative pressure than men. J Appl Physiol 1996;80(4):1138-1143. 12. Morikawa T, Sagawa S, Torii R, Endo Y, Yamazaki F and Shiraki K. Hypovolemic intolerance to lower body negative pressure in female runners. Med Sci Sports Exerc 2001;33(12):20582064. 13. Howley ET, Basset DR and Welch HG. Criteria for maximal oxygen uptake: review and commentary. Med Sci Sports Exerc 1995;27(9):1292-1301. 14. Hernandez JP and Franke WD. Age-and fitness-related differences in limb venous compliance do not affect tolerance to maximal lower body negative pressure in men and women. J Appl Physiol 2004;97(3):925-929. 15. Halliwill JR, Minson CT and Joyner MJ. Measurement of limb venous compliance in humans: technical considerations and physiological findings. J Appl Physiol 1999;87(4):1555-1563. 16. Lanne T and Olsen H. Decreased capacitance response with age in lower limbs of humans: a potential error in the study of cardiovascular reflexes in ageing. Acta Physiol Scand 1997;161:503-507. 17. Schnizer W, Klatt J, Baeder H and Rieckert H. Comparison of scintigraphic and plethysmographic measurements for determination of capillary filtration coefficient in human limbs. Basic Res Cardiol 1978;73:77-84. 18. Lindenberger M and Lanne T. Sex-related effects on venous compliance and capillary filtration in the lower limb. Am J Physiol Regul Integr Comp Physiol 2007;292(2):R852R859. Tanaka H, Dinnenno FA, Monahan KD, Clevenger CM, De Souza CA and Seals DR. Aging, habitual exercise, and dynamic arterial compliance. Circulation 2000;102(11):1270-1275. 19. 20. Halliwill JR, Lawler LA, Eickhoff TJ, Joyner MJ and Mulvagh SL. Reflex responses to regional venous pooling during lower body negative pressure in humans. J Appl Physiol 1998;84(2):454-458. 21. Oren S, Grossman E. and Frohlich ED. Arterial and venous compliance in obese and nonobese subjects. Brief Reports. Am J Cardiol 1996;77:665-667. 22. Stepniakowski K and Egan BM. Additive effects of obesity and hypertension to limit venous volume. Am J Physiol 1995;268(2 Pt 2):R562-R568. 23. Karas RH, Patterson BL, and Mendelsohn ME. Human vascular smooth muscle cells contain functional estrogen receptors. Circulation 1994;89(5):1943-1950. 24. Mendelsohn ME. Genomic and nongenomic effects of estrogen in the vasculature. Am J Cardiol 2002;90(1A):3F-6F. Venous Compliance in Trained Females 49 Disclaimer The opinions expressed in JEPonline are those of the authors and are not attributable to JEPonline, the editorial staff or ASEP.