INITIAL - nndhealthcare.com
advertisement

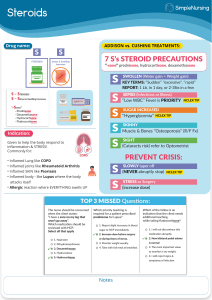
Prednisone PATIENT NAME ___________________________________ SOC _______________ INITIAL Action of prednisone. ______ ______ A. To decrease inflammation. ______ ______ B. For replacement therapy in adrenalcortical deficiency. Possible adverse reactions. ______ ______ A. Headache. ______ ______ B. Nausea/vomiting. ______ ______ C. Acne. ______ ______ D. Appetite increase or decrease. ______ ______ E. Delayed wound healing. ______ ______ F. Dizziness. ______ ______ G. Urination at night time. ______ ______ H. Insomnia. ______ ______ I. Headache. ______ ______ J. Muscle weakness. ______ ______ K. Weight gain. ______ ______ L. High blood pressure. ______ ______ M. Fever. ______ ______ N. Fatigue. ______ ______ O. Back or rib pain. ______ ______ P. Abdominal pain. ______ ______ Q. Bloody or tarry stools. ______ ______ R. Allergic reaction. Precautions when taking prednisone. ______ ______ A. Take prednisone with food or milk to decrease gastric distress. ______ ______ B. Follow a salt-restricted diet that is high in potassium and protein as ordered. ______ ______ C. Weigh daily and report any sudden increase to physician. ______ ______ D. Never stop taking abruptly, but discontinue it gradually, decreasing doses as ordered. (May be fatal if stopped abruptly.) ______ ______ E. Withdrawal symptoms include rebound inflammation, fatigue, weakness, arthralgia, fever, dizziness, lethargy, depression, fainting, orthostatic hypotension, dyspnea, anorexia. ______ ______ F. Give once-daily doses in the morning for less toxicity. ______ ______ G. Avoid over-the-counter medications without approval from physician, especially those with aspirin, sodium, or alcohol. ______ ______ H. Wear a Medic Alert bracelet. ______ ______ I. Exercise daily to decrease possibility of osteoporosis. ______ ______ J. Steroids may decrease contraceptive action of oral contraceptives. ______ ______ K. Report any signs of slow healing. (Prednisone may mask or exacerbate infections.) ______ ______ L. Perform measures to prevent infection because of increased susceptibility: 1 Prednisone PATIENT NAME ___________________________________ SOC _______________ ______ ______ 1. Avoid crowds or contact with people with infections. ______ ______ 2. Provide good hygiene and cleanliness. ______ ______ 3. Provide good foot care. ______ ______ M. Report any signs of hyperglycemia, i.e., sweating, shakiness, fruity odor of breath, etc. ______ ______ N. Report any early signs of adrenal insufficiency, i.e., fatigue, muscular weakness, joint pain, fever, anorexia, nausea, dyspnea, dizziness, fainting, etc. ______ ______ O. Report any signs of cushingoid symptoms if on long-term dosage, i.e., facial or visual changes, easy bruising, amenorrhea, edema, humpback, etc. ______ ______ P. Report any signs of depression or psychotic episodes while taking high dose therapy. ______ ______ Q. Keep follow-up appointments with physician. 2