Outpatient Order Imaging Services
advertisement

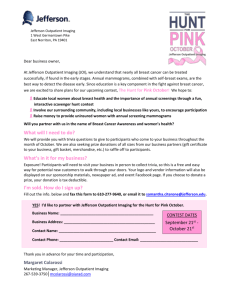
PLACE LABEL HERE OUTPATIENT ORDER IMAGING SERVICES Imaging Scheduling: Phone: 678-312-3444 Fax: 678-442-9736 Precertification: 678-312-4095 Location of Scheduled Appointment: Gwinnett Medical Center – Lawrenceville Gwinnett Women’s Pavilion 575 Outpatient Imaging Center Gwinnett Medical Center – Duluth Outpatient Center at GMC – Duluth GMC Imaging Center – Hamilton Mill GHS to Schedule Patient? Yes No Patient already scheduled? Yes No Appointment Date: _________________ Arrival Time: ______________________ Exam Time: _______________________ Medicare? Yes No GMC to Precert Patient? Yes No *If yes, copy of insurance card & clinical documentation must be sent with order* Precertification # : ______________________ Allergies: _______________________________________________________________________ Name: DOB: __________________________ _________________________ Phone#1: _________________________ Phone#2: _________________________ Language: _________________________ PATIENT MUST BRING THIS ORDER ON THE DATE OF SERVICE. ALL FLUOROSCOPY & ULTRASOUND PROCEDURES MUST BE SCHEDULED. Symptoms/Diagnosis (with ICD-9 codes): ______________________________________________________________________________________ ________________________________________________________________________________________________________________________ IMAGING WILL EVALUATE CREATININE LEVEL PRIOR TO CONTRASTED TESTS UNLESS LAST LEVEL PERFORMED WITHIN 7DAYS. DATE / RESULT:_________________________________ SKULL & FACE Skull Series Facial Bones Orbits: Rt Lt Nasal Bones Sinus Series: Full Series Limited Other: ______________ CHEST Chest: PA & Lateral Decubitus: Rt Lt Bilateral Ribs: Rt Lt Bilateral Sternum Other: ______________ SPINE & PELVIS Cervical Spine Thoracic Spine Lumbar Spine Pelvis Sacroiliac Joint Hip: Rt Lt Bilateral Sacrum and/or Coccyx specify: _____________ Scoliosis Series Other: _______________ EXTREMITIES Rt Lt Bilateral Specify site: ____________ Bone Length Scanogram Standing / Weight-Bearing Bone Age Other: _______________ GU TRACT Cystogram: Static Voiding IV Pyelogram with Post Void Other:________________ ABDOMEN & GI TRACT Acute Abdominal Series Barium Enema: Single Air Contrast Barium Swallow (esophagus) Modified Barium Swallow KUB Small Bowel Series Upper GI Series Other: ______________ OTHER PROCEDURES Arthrogram: (with Contrast) Specify: ______________ Rt Lt with MRI with CT Hip Injection: Rt Lt Hysterosalpingogram Myelogram with CT to follow: Cervical Thoracic Specify level: ___________ Lumbar Other: _______________ ULTRASOUND Abdomen Complete Abdomen Limited Specify site : ____________ Aorta Kidneys Paracentesis: OB Pelvis OB Transvaginal EDD ___________LMP _________ Pelvic Non-OB (transvaginal & transabdominal) Transvaginal ONLY Transabdominal ONLY Retroperitoneum (AA, IVC) Sonohysterogram Testicular Thoracentesis: Rt Lt Thyroid Thyroid Biopsy: Rt Lt Bilateral Venous Upper Extremity: Rt Lt Bilateral Venous Lower Extremity: Rt Lt Bilateral Other: ________________ Physician Name (print): ____________________________________ STAT Results to: Phone Fax: __________________________ Physician Signature: ______________________________________ Hold patient and Call Physician’s cell: ________________________ Physician NPI#: ______________________Date: _______________ CC report to: ___________________________________________ *2-18692* 2 FORM 2-18692 REV. 02/2012 WHITE: Medical Record CANARY: Physician Office Page 1 of PLACE LABEL HERE OUTPATIENT ORDER IMAGING SERVICES For directions, go to WWW.GWCIMAGING.ORG and click onto the facility where you are scheduled. Gwinnett Medical Center - Duluth 3620 Howell Ferry Road Duluth, Georgia 30096 phone: 678-312-6693 Gwinnett Medical Center 1000 Medical Center Boulevard Lawrenceville, Georgia 30046 phone: 678-312-4440 Outpatient Center at Gwinnett Medical Center - Duluth 3805 Pleasant Hill Road Duluth, Georgia 30096 phone: 678-312-7000 575 Outpatient Imaging Center 575 Professional Drive, Suite 400 Lawrenceville, Georgia 30046 phone: 678-312-5300 GMC Imaging Center – Hamilton Mill 2078 Teron Trace, Suite 200 Dacula, GA 30019 phone: 678-312-8600 GMC PET/CT & 3T MRI 631 Professional Drive, Suite 190 Lawrenceville, Georgia 30046 phone: 678-312-5300 *PET/CT & MRI ONLY* FORM 2-18692 REV. 02/2012 Page 2 of 2