PCA Order Form: Morphine & Dilaudid Dosage Guidelines
advertisement

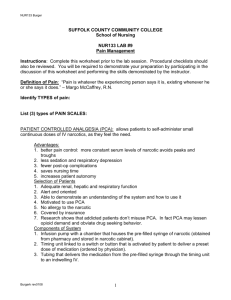
PLACE LABEL HERE PATIENT CONTROLLED ANALGESIA (PCA) ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). Drug (concentration) Use Initial loading dose PCA demand dose PCA lockout interval 4 hour dose limit Continuous rate Supplemental bolus dose PCA Medication: Morphine (1 mg/ml) Dilaudid (HYDROmorphone) (0.2 mg/ml) Most patients; Caution with poor renal function 1–2 mg Patients unable to be managed with morphine 0.5–1 mg 1–2 mg 6–10 min Usual 20 mg Maximum 30 mg 0.5-2 mg/hr 1-2 mg Maximum 5 doses in 4 hrs Morphine 0.2–0.4 mg 6–10 min Usual 4 mg Maximum 6 mg 0.1-0.5/hr 0.25-0.5 mg Maximum 5 doses in 4 hrs Dilaudid (HYDROmorphone) 1. 2. 3. 4. 5. 6. 7. Initial loading dose (prior to starting PCA): _______________ mg IV x 1 dose Mode of delivery: PCA only Continuous only PCA + continuous PCA demand dose: _________________________________________ mg PCA lockout interval: ________________________________________ min Four hour dose limit: ________________________________________ mg Continuous rate (if applicable): ________________________________ mg/hr Supplemental IV bolus doses: If Morphine PCA, give: Morphine 1-2 mg IV (not PCA) If Dilaudid (HYDROmorphone) PCA, give: HYDROmorphone 0.25-0.5 mg IV (not PCA) Repeat q 15 min prn pain. Do not exceed 5 doses in 4 hrs 8. Discontinue PCA : in 12 hrs in 24 hrs POD 1 at 0600 POD 2 at 0600 When ordered to do so by provider OTHER MEDICATIONS 9. IV fluids: As per previous physician orders or ______________ IV at ______ ml/hr for PCA line 10. If CNS or respiratory depression occurs (LOS Score = 4 and respiratory rate ≤ 8): Narcan (naloxone) 0.4 mg diluted in NS 10 ml (0.04 mg/ml), administer 1 ml q 2 min until LOS Score = 2 and respiratory rate > 10, Notify physician Sedation Scale: 0 - Awake, alert 1 - Occasionally drowsy, easy to arouse 2 - Frequently drowsy or normal sleep, easy to arouse 3 - Somnolent, difficult to arouse 4 - Obtunded, unable to arouse ________________ _______________ Date Time *1-2119* 1 _________________________________ Physician Signature FORM 1-2119 REV. 05/2015 WHITE: Medical Record ___________ PID Number CANARY: Pharmacy Page 1 of

![See our handout on Classroom Access Personnel [doc]](http://s3.studylib.net/store/data/007033314_1-354ad15753436b5c05a8b4105c194a96-300x300.png)