Division of Medical Assistance
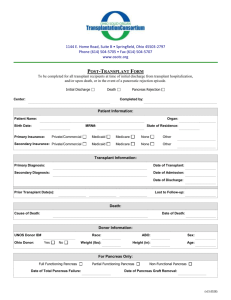
Pancreas Transplant
NCHC Policy No.: NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
Table of Contents
1.0
Description of the Procedure, Product, or Service ........................................................................... 1
1.1
Clinical Situations for Consideration of Pancreas Transplantation. ................................... 1
1.2
Medical Term Definitions ................................................................................................... 2
2.0
Eligible Recipients ........................................................................................................................... 2
2.1
General Provisions .............................................................................................................. 2
3.0
When the Procedure, Product, or Service Is Covered ...................................................................... 2
3.1
General Criteria................................................................................................................... 2
3.2
Specific Criteria .................................................................................................................. 3
4.0
When the Procedure, Product, or Service Is Not Covered ............................................................... 4
4.1
General Criteria................................................................................................................... 4
4.2
Specific Criteria .................................................................................................................. 4
5.0
Requirements for and Limitations on Coverage .............................................................................. 5
5.1
Prior Approval .................................................................................................................... 5
6.0
Providers Eligible to Bill for the Procedure, Product, or Service .................................................... 5
7.0
Additional Requirements ................................................................................................................. 5
7.1
Compliance ......................................................................................................................... 5
8.0
Policy Implementation/Revision Information .................................................................................. 5
Attachment A: Claims-Related Information ................................................................................................. 6
A.
Claim Type ......................................................................................................................... 6
B.
Diagnosis Codes ................................................................................................................. 6
C.
Procedure Code(s)............................................................................................................... 6
D.
Modifiers............................................................................................................................. 6
E.
Billing Units........................................................................................................................ 6
F.
Place of Service .................................................................................................................. 6
G.
Co-payments ....................................................................................................................... 6
H.
Reimbursement ................................................................................................................... 6
05.10.2010 – PAG Submission
i
Division of Medical Assistance
Pancreas Transplant
1.0
NCHC Policy No.: NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
Description of the Procedure, Product, or Service
This policy covers three different transplantation services:
a. simultaneous pancreas and kidney transplant;
b. pancreas transplant some time following a kidney transplant; and
c. pancreas transplant alone.
The pancreas is an organ in the abdomen that is vital in the digestive process of the body. The
pancreas secretes digestive enzymes, and hormones one of which is insulin. Insulin regulates the
carbohydrate metabolism in the body.
Transplantation of a normal pancreas is a treatment method for recipients with diabetes mellitus.
Pancreas transplantation can restore glucose control and is intended to prevent, halt, or reverse the
secondary complications of type 1 diabetes mellitus. Diabetes mellitus is a metabolic disorder in
which the body cannot oxidize carbohydrates, usually due to faulty pancreatic activity and a
disturbance in the normal insulin mechanism.
The primary goal of pancreas transplantation is to provide insulin independence, decrease
morbidity, and increase the quality of life for a recipient with diabetes. While pancreas
transplantation is generally not considered a life-saving treatment, it can be life-saving in a small
subset of recipients who experience life-threatening complications from type 1 diabetes mellitus.
1.1
Clinical Situations for Consideration of Pancreas Transplantation.
Pancreas transplantation may be considered in several different clinical situations such
as:
a. a type 1 diabetic recipient with renal failure who may receive a cadaveric
simultaneous pancreas/kidney transplant (SPK);
b. a type 1 diabetic recipient who may receive a cadaveric or living-related pancreas
after a kidney transplantation (pancreas after kidney, i.e., PAK);
c. a non-uremic type 1 diabetic recipient with specific severely disabling and potentially
life-threatening diabetic problems who may receive a pancreas transplant alone
(PTA).
The experience with SPK transplant is more extensive than that of other transplant
options.
The approach to re-transplantation varies according to the cause of failure.
Surgical/technical complications such as venous thrombosis are the leading cause of
pancreatic graft loss among diabetic recipients. Graft loss from chronic rejection may
result in sensitization, increasing both the difficulty of finding a cross-matched donor
and the risk of rejection of a subsequent transplant.
CPT codes, descriptors, and other data only are copyright 2010 American Medical Association. All rights
reserved. Applicable FARS/DFARS apply.
05.10.2010 – PAG Submission
1
Division of Medical Assistance
Pancreas Transplant
1.2
NCHC Policy No. NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
Medical Term Definitions
a. Cadaver donor: an organ or tissue from a dead body.
b. Cardiopulmonary: pertaining to the heart and lungs.
c. Hypoglycemia: an abnormally low level of glucose in the blood.
d. Insulin: the major fuel regulating hormone produced by the pancreas. It is secreted by
the pancreas into the blood in response to a rise in the concentration of glucose in the
blood. It promotes the storage of glucose in the liver, skeletal muscle, and fatty
tissue, increases protein synthesis, and prompts other vitalmetabolic body functions.
e. Kidney: two glands shaped like two large beans that act as a filter of the blood and
control the level of some chemicals in the blood such as hydrogen, sodium,
potassium and phosphate. They also eliminate waste in the form of urine.
f.
Labile: fluctuating; unstable.
g. Malignant: cancerous, not benign; describes a tumor that invades and destroys the
tissues in which it originates and can spread to other sites in the body via the
bloodstream and lymphatic system. If untreated, these tumors cause progressive
deterioration and death.
h. Morbidity: a diseased condition; the incidence or prevalence of a disease or of all
diseases in a population.
i.
Non-uremic: absence of excessive by-products of protein metabolism in the blood
and resulting toxic condition.
j.
Renal: pertains to the kidneys.
k. Uremia (uremic): the retention of excessive by-products of protein metabolism in the
blood and the resulting toxic condition.
2.0
Eligible Recipients
2.1
General Provisions
To be eligible, NCHC recipients must be enrolled on the date of service.
3.0
When the Procedure, Product, or Service Is Covered
3.1
General Criteria
NCHC covers procedures, products, and services related to this policy when they are
medically necessary and
a.
the procedure, product, or service is individualized, specific, and consistent with
symptoms or confirmed diagnosis of the illness or injury under treatment, and not
in excess of the recipient’s needs;
b.
the procedure, product, or service can be safely furnished, and no equally effective
and more conservative or less costly treatment is available; AND
05.10.2010 – PAG Submission
2
Division of Medical Assistance
Pancreas Transplant
c.
3.2
NCHC Policy No. NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
the procedure, product, or service is furnished in a manner not primarily intended
for the convenience of the recipient, the recipient’s caretaker, or the provider.
Specific Criteria
Pancreas transplantation, (a pancreas alone, simultaneous with a kidney transplant, or
following a kidney transplant) may be covered under the NC Health Choice Program
when it is determined to be medically necessary because the following medical criteria
are met.
a. Candidates for any type of pancreas transplant should meet ALL of the following
criteria:
1. Adequate cardiopulmonary status;
2. Absence of active infection;
3. Absence of uncontrolled HIV infection. HIV infection is considered controlled
when the following criteria are met:
(a)
the CD4 count >200 cells/mm-3 for > 6 months; and
(b)
the HIV-1 RNA undetectable;
(c)
the recipient is stable on anti-retroviral therapy > 3 months; and
(d)
the recipient has no other complications from AIDS (e.g., opportunistic
infection, including aspergillus, tuberculosis, coccidioses mycosis,
resistant fungal infections, Kaposi’s sarcoma, or other neoplasm;
4. No history of malignancy within 5 years of transplantation, excluding
nonmelanomatous skin cancers; and
5. Documentation of recipient compliance with medical management.
b. Candidates for pancreas transplant alone should additionally meet ONE of the
following severity of illness criteria:
1. documentation of severe hypoglycemia unawareness as evidence by chart notes
or emergency room visits; OR
2. documentation of potentially life-threatening labile diabetes as evidenced by
chart notes or hospitalization for diabetic ketoacidosis.
c. Listed below are the clinical indications for the three (3) types of pancreas
transplants:
1. Combined pancreas-kidney transplant may be considered medically necessary in
diabetic recipients with uremia.
2. Pancreas transplant after a prior kidney transplant may be considered medically
necessary in recipients with insulin dependent diabetes mellitus.
3. Pancreas transplant alone may be considered medically necessary in recipients
with severely disabling and potentially life-threatening complications due to
hypoglycemia (abnormally low level of glucose in the blood) unawareness and
labile diabetes that persists in spite of optimal medical management.
05.10.2010 – PAG Submission
3
Division of Medical Assistance
Pancreas Transplant
NCHC Policy No. NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
4. Pancreas re-transplant after a failed primary pancreas transplant may be
considered medically necessary for all three types of pancreas transplants (i.e.,
combined pancreas-kidney transplant, pancreas transplant after a prior kidney
transplant, and pancreas transplant alone).
4.0
When the Procedure, Product, or Service Is Not Covered
4.1
General Criteria
Procedures, products, and services related to this policy are not covered when
a.
the recipient does not meet the eligibility requirements listed in Section 2.0;
b.
the recipient does not meet the medical necessity criteria listed in Section 3.0;
c.
the procedure, product, or service unnecessarily duplicates another provider’s
procedure, product, or service; or
d.
the procedure, product, or service is experimental or investigational.
4.2
Specific Criteria
a. Pancreas transplantation is not covered for:
1. indications other than those cited in Subsection 3.2.
2. organs sold rather than donated to a recipient.
3. artificial organs or human organ transplant service for which the cost is covered
or funded by governmental, foundation, or charitable grants.
b. Contraindications for the combined pancreas/kidney transplantation include the
following:
1. poor physiologic age;
2. significant emotional problems that may impair the recipient’s ability to adhere
to follow-up;
3. recent substance abuse;
4. current tobacco use (impairs wound and microvascular healing);
5. history of non-compliance with medical management;
6. lack of support to the extent that adequate follow-up and adherence to post
operative treatment plan is impaired;
7. other major organ system disease or infection, including major vascular disease;
8. morbid obesity; and
9. uncontrolled HIV positive recipients.
05.10.2010 – PAG Submission
4
Division of Medical Assistance
Pancreas Transplant
5.0
NCHC Policy No. NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
Requirements for and Limitations on Coverage
5.1
Prior Approval
Prior approval is required for all transplants, including pancreas transplantation. Only
those recipients accepted for transplantation by an approved transplantation center and
actively listed for transplant should be considered for prior approval.
6.0
Providers Eligible to Bill for the Procedure, Product, or Service
To be eligible to bill for procedures, products, and services related to this policy, providers shall
a. meet NCHC qualifications for participation;
b. be currently enrolled with NCHC; AND
c. bill only for procedures, products, and services that are within the scope of their clinical
practice, as defined by the appropriate licensing entity.
7.0
Additional Requirements
7.1
Compliance
Providers must comply with all applicable federal, state, and local laws and regulations,
including the Health Insurance Portability and Accountability Act (HIPAA) and record
retention requirements.
8.0
Policy Implementation/Revision Information
Original Effective Date: July 1, 2010
Revision Information:
Date
July 1, 2010
Section Revised
05.10.2010 – PAG Submission
Change
Policy Conversion: Implementation of Session
Law 2009-451, Section 10.32 “NC HEALTH
CHOICE/PROCEDURES FOR CHANGING
MEDICAL POLICY.”
5
Division of Medical Assistance
Pancreas Transplant
NCHC Policy No. NCHC2010.062
Original Effective Date: July 1, 2010
Revised Date:
Attachment A: Claims-Related Information
Reimbursement requires compliance with all NCHC guidelines.
A. Claim Type
Professional (CMS-1500/837P transaction)
Institutional (UB-04/837I transaction)
B. Diagnosis Codes
Providers must bill the ICD-9-CM diagnosis codes(s) to the highest level of specificity that
supports medical necessity.
C. Procedure Code(s)
CPT Codes
48160
48550
48551
48552
48554
48556
50300
50320
HCPCS Codes
S2065
S2152
If prior approval has not been obtained, claims will deny.
D. Modifiers
Providers are required to follow applicable modifier guidelines.
E. Billing Units
The appropriate procedure code(s) used determines the billing unit(s).
F. Place of Service
Inpatient Hospital
G. Co-payments
Co-payment(s) may apply to covered prescription and services.
H. Reimbursement
Providers must bill their usual and customary charges.
05.10.2010 – PAG Submission
6