Oscillatory Devices for Airway Clearance including High
advertisement

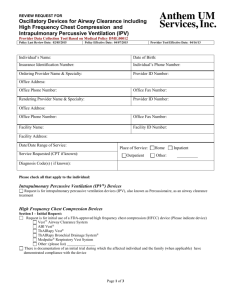
REVIEW REQUEST FOR Oscillatory Devices for Airway Clearance including High Frequency Chest Compression (Vest™ Airway Clearance System) and Intrapulmonary Percussive Ventilation (IPV) Provider Data Collection Tool Based on Medical Policies 1.01.15; DME.00012 1.01.15 Policy Last Review Date: 12/7/2011 DME.00012 Policy Last Review Date: 02/17/2011 1.01.15 Policy Effective Date: 01/01/2012 Policy Effective Date: 04/13/2011 Provider Tool Effective Date: 03/22/2011 Member Name: Date of Birth: Insurance Identification Number: Member Phone Number: Ordering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Rendering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Facility Name: Facility ID Number: Facility Address: Date/Date Range of Service: Place of Service: Service Requested (CPT if known): Outpatient Home Inpatient Other: Diagnosis (ICD-9) if known): Please check all that apply to the member: Type of Oscillatory Device The Bird IPV® Noncontinuous Ventilator FLUTTER® Mucus Clearance Device The ThAIRapy Bronchial Drainage System or Vest™ Airway Clearance System The Acapella® device The RC Cornet™ Mucus Clearing Device Other Device ______________________________ The member has: (Check all that apply) Documented need of airway clearance Cystic fibrosis (CF) Chronic bronchiectasis Chronic neuromuscular disorder affecting the ability to cough or clear respiratory secretions and prior history of pneumonia or other significant worsening of pulmonary function Documentation of failure of other methods or inability to use other airway clearance therapies including chest physical therapy due to: (Check all that apply) Two or more children with cystic fibrosis in the family Inability of the caregiver [physical or mental] to perform chest physical therapy at the required frequency No availability of parental or partner resource to perform chest physical therapy Page 1 of 2 REVIEW REQUEST FOR Oscillatory Devices for Airway Clearance including High Frequency Chest Compression (Vest™ Airway Clearance System) and Intrapulmonary Percussive Ventilation (IPV) Provider Data Collection Tool Based on Medical Policies 1.01.15; DME.00012 1.01.15 Policy Last Review Date: 12/7/2011 DME.00012 Policy Last Review Date: 02/17/2011 1.01.15 Policy Effective Date: 01/01/2012 Policy Effective Date: 04/13/2011 Provider Tool Effective Date: 03/22/2011 Other: (please list) Member has history of : (check all that apply) Unstable head or neck injury Active hemorrhage with hemodynamic instability Subcutaneous emphysema Recent epidural, spinal fusion, or spinal anesthesia Recent skin grafts or flaps Burns, open wounds and skin infections of the thorax Recently placed transvenous pacemaker or subcutaneous pacemaker Suspected pulmonary tuberculosis Lung contusion Bronchospasm Osteomyelitis of the ribs Osteoporosis Coagulopathy Complaint of significant chest wall pain Chronic obstructive pulmonary disease Other: (please list) Section II – Continued Use Request: (SECTION I MUST ALSO BE COMPELTED) Request is for approval after initial trial or extension of previous authorization There is affected member/family compliance with the device as evidenced by an initial trial period and: (Check all that apply) This is monitored by a report at 6-12 months interval which reviews monthly usage of device (for device with usage meters) The report documents sufficient use to be clinically effective (67% or more of the prescribed time) Other: (please list) Request is for alternative method of airway clearance as a result of intolerance to the device or failure to comply with usage meter checks. Please describe: Other: (please list) This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I attest the information provided is true and accurate to the best of my knowledge. I understand that Anthem may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. _____________________________________________________________ Name and Title of Provider or Provider Representative Completing Form and Attestation (Please Print)* Date *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Page 2 of 2