Medication and Treatment Administration Form
advertisement

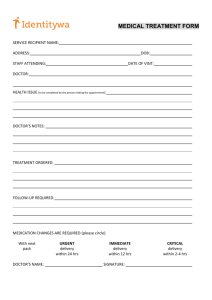
Heartwood School Medication and Treatment Administration Form Attention PARENT/GUARDIAN/ or GROUP HOME MGR: Please complete the TOP SECTION (ONLY) and return the form to the Heartwood School Clinic. STUDENT NAME:_______________________________________________ BIRTHDATE:__________________ Medication Dose/Amount Time(s) given @ school Time(s) given @ home Please check any over-the-counter (OTC) medications (below) that your student may receive at school. We request permission to administer these OTC meds. when the student needs them. This prevents delays in symptom relief. Tylenol/Acetaminophen tablet/elixir, per student weight, every 4-6 hours. as needed (PRN) for fever or discomfort Ibuprofen/Motrin tablet/elixir, per student weight, every 4-6 hours. as needed (PRN) for fever or discomfort Benadryl/Diphenhydramine, 12.5mg–25mg per student weight., 4-6 hrs. PRN for allergy-type symptoms Doctor’s Name & Phone: ___________________________________________________________ I hereby authorize Heartwood School to administer the medication(s) and or treatment(s)as prescribed. Parent/Guardian/Resident Mgr. Signature: ____________________________________ Date:________________ Parent/guardian – STOP HERE, please. The School Nurse will forward it to the doctor to sign. *********************************************************************************** DOCTOR or NURSE to review or edit medications/treatments and return to Heartwood School Clinic. DOCTOR/NURSE to sign below and return by FAX to: 517 676-5302 or mail to: Heartwood School Nurse 625 Hagadorn Road Mason MI 48854 Attn: R.N. at Heartwood School Clinic Phone (517) 244-1420 DOCTOR’S ORDERS: Type(s) of medication or treatment and the dosage is to be given in the amount of tablets/capsules/teaspoons/ cc’s/ml’s daily or as follows: Possible Side Effects: _________________________________________________________________________ Duration: Current School Year Other:_____________________________________________________ The Registered Nurse at Heartwood School has permission to give medication or treatment as directed above. Doctor’s Signature: Date: ______________________ Forms/Medication & Treatment Form NEW