Clinical Engineering - Institute of Industrial Engineers
advertisement

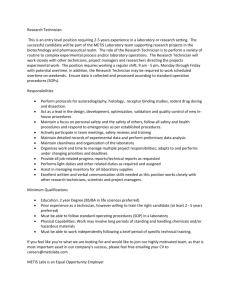
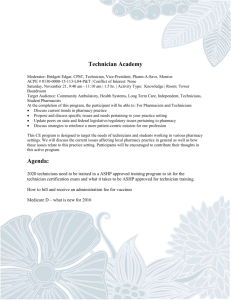
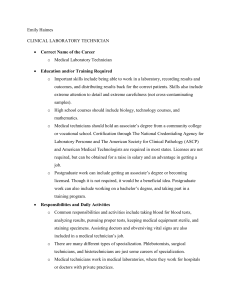
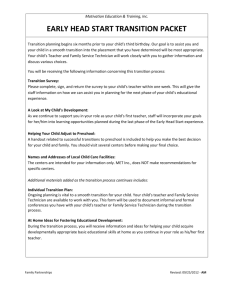
MOUNT SINAI MEDICAL CENTER CLINICAL ENGINEERING DEPARTMENT REVIEW By Christopher Maloney Abstract A Clinical Engineering department is among the most important support departments that a hospital can have. Clinical Engineering is responsible for the maintenance and repair of all medical support equipment on a medical campus. They must use their training and experience to be able to troubleshoot and solve almost any problem with medical equipment that a medical staff may encounter during the course of a day. Some of their other responsibilities include building knowledge on the current trends in medical equipment, as well as constantly training to stay updated as equipment gets upgraded. All these responsibilities can be summarized by saying that Clinical Engineering is responsible for ensuring that medical equipment is in good working order and helping the hospital make important decisions on new equipment. In order to get a detailed look at the operations of the Clinical Engineering department at Mount Sinai Medical Center, I was asked to perform a departmental review. The purpose of this project was to develop a thorough understanding of the processes of the Clinical Engineering department to see that they are operating effectively and if there is any room to improve. To learn about the department, I spent six weeks shadowing different employees to see what their different jobs were and how they interacted with the other employees and went about doing their jobs. The following is a detailed report on what I was able to find during this six week period. Aramark The responsibilities of the Clinical Engineering department at Mount Sinai Medical Center are outsourced to a company called Aramark. Aramark is a large, international company, headquartered in Philadelphia, PA, that provides professional services which include food services, facilities management, and uniform apparel to businesses around the world. ("About aramark,") These services are provided to companies in nearly every industry including public safety, entertainment, convention centers, and healthcare. The Aramark branch that Mount Sinai deals with is the Clinical Technology Services branch. The office that serves Mount Sinai is located in the Miami Heart Institute. At Mount Sinai, they have two separate departments; biomedical engineering and imaging. The biomedical engineering department is located on the ninth floor of the Blum building on Mount Sinai’s main campus. The imaging department is located on the second floor of the main building on Mount Sinai’s main campus. Department Overview The Clinical Engineering department at Mount Sinai Medical Center is responsible for everything involving medical equipment owned by the hospital. Their two main tasks include preventive maintenance and broken equipment repair, but their work extends beyond that. Some of the other tasks that the Clinical Engineering department is responsible for include new or alternative equipment recommendations, new equipment inspections, daily Operating Room rounds and hospital moves. Service Calls Service calls are the major responsibility of the Clinical Engineering department is responsible for. Any employee in the hospital can call the department when a piece of medical equipment is not functioning properly and expect that it will be fixed within a reasonable time period. This function is especially important in the event that equipment is not working before or during a surgical procedure to ensure patient safety. Preventive Maintenance In order to prevent incidents, equipment failure, and to meet Joint Commission standards, the Clinical Engineering department performs preventive maintenance on nearly all of the equipment that it is responsible for. The first thing the employee performing the maintenance always does is clean the equipment with alcohol wipes. Then, they will perform tasks ranging from electrical safety tests to checking the fluid levels of the machine. If anything is found to be wrong with the machine during the preventive maintenance inspection, it is fixed before the machine can be used again. New Equipment Recommendations It is the job of the Clinical Engineering department to stay up on current trends in medical equipment nationwide so that when called upon for advice in purchasing new equipment, they can provide sound advice. It is also the job of the staff to evaluate the condition of the current equipment as they perform maintenance and make recommendations for new equipment if the old equipment is obsolete or going to be obsolete in the near future. Incoming Equipment Inspections When new equipment arrives at the hospital, Clinical Engineering must be informed by the Shipping and Receiving Department. Clinical Engineering then goes to pick up the equipment and perform an incoming inspection before releasing the equipment to the floor. Incoming inspections usually consist of various safety tests and giving the new equipment an asset number. The final employee located in Miami Heart Institute is a technician responsible for maintaining and servicing all of the equipment at the Miami Heart campus, as well as assisting the biomedical technicians at the Mount Sinai campus. Due to the small amount of equipment still located at Miami Heart, this technician does spend about 10 hours every week assisting the biomedical technicians at the Mount Sinai main campus. Daily Rounds Every morning around 7:30, one technician is sent to make the daily rounds. This entails going to the main Operating Room, the Ambulatory Center, Central Services, and the Operating Room overflow area to make sure that all of the equipment is working as well as it is supposed to in order to make sure the cases can all flow smoothly throughout the day. When the Clinical Engineering department gets itself back to being fully staffed, they plan on doing rounds on every floor at least once during the week. Mount Sinai Medical Center Biomed Department The Biomed Department of Clinical Engineering has gone through some major staffing changes. At the moment, they are understaffed as they have lost some employees to military obligations and relocations. When fully staffed, the Biomed Department consists of seven technicians. Of these seven technicians, one constantly works on preventive maintenance and repairing equipment in the shop. The rest of the technicians spend time doing preventive maintenance as well as taking service calls. Additionally, one technician every week is designated as the on-call technician who must be available 24 hours a day for that week in case some essential equipment malfunctions during the night time or weekend hours. Currently there are five technicians on staff. Three of the technicians are rotating between working on preventive maintenance and service calls. One technician is working primarily on preventive maintenance and repairs. One technician was recently hired and is doing preventive maintenance as he learns his way around the hospital. After he has become more familiar with where everything in the hospital is located, his responsibilities will grow to include taking service calls as well. Hospital Moves When a department moves within the hospital, Clinical Engineering is called upon to move and set up any medical equipment that is required in the new location. They then monitor the equipment to make sure it is functioning properly as the patients are moved to the new location. Other Tasks Among the regular tasks listed above, Clinical Engineering also is responsible for projects that come up periodically. Some of the projects they worked on during the observation period included replacing batteries in monitors with newer models after the failure of some older models, assisting vendors with possible recalls, and teaching hospital employees how to use certain equipment functions. Staffing Miami Heart Institute At Miami Heart Institute, Aramark has 4 employees. The first employee is the supervisor in charge of the Clinical Engineering operations at Mount Sinai. His responsibilities are all business related and he communicates with headquarters, his district manager, as well as Mount Sinai executives. He has experience in the biomedical field and has moved into a management role. Also employed in the office at Miami Heart are two clerical employees. These two employees are responsible for directing phone calls, payroll, basic accounting, printing work orders for preventive maintenance, filing all work orders, and maintaining their equipment database. They appear to be very busy at all times and have very crucial jobs to the functionality of the department. Mount Sinai Medical Center Imaging Department The Imaging Department of Clinical Engineering consists of 2 employees. The first of these employees is a supervisor. His responsibilities include hospital related tasks such as maintaining equipment, managing service contracts with outside vendors, coordinating service and preventive maintenance with hospital department supervisors, and making recommendations for new equipment purchases. Additionally, the supervisor is involved in two committees outside of Mount Sinai Medical Center. The first is the Quality Standards Committee and the other is the Imaging Sub Committee of which he is the president. Both of these committees’ goals are to improve the quality of service Aramark provides its customers and to create standard practices in the imaging departments nationwide. The second employee in the imaging department is more of a technician. His main job is to repair and perform maintenance on equipment. He is also responsible for helping outside service vendors when they come to the hospital to repair equipment. -2- Staff Personalities The members of the Clinical Engineering department all seemed to interact well with hospital staff. They all seemed to have a “patients come first” attitude about everyday issues that they faced, and this attitude was reinforced by the supervisors whenever necessary. The technicians all seemed to have a sense of pride about their work and would not put a piece of equipment out on the floor unless they knew for a fact that it was going to be functional. Policies Staffed Hours The department is responsible for having technicians in the hospital from 7:00 A.M. until 5:00 P.M. Monday through Friday. In addition, they must have an employee on call 24 hours a day to cover any non-regular hours. The employees come in for work at different times ranging from 7:00 A.M. to 9:00 A.M. to cover their time window. They are expected to work eight hours a day with a one hour break for lunch, although most of the time they stay beyond the eight hours to make sure the equipment is maintained on time. Preventive Maintenance All preventive maintenance work orders are issued on the first day of a particular month. The department goal for all preventive maintenance is to have the work order completed within 30 days of being issued. Life support equipment is required to be completed within those 30 days. All other equipment must be completed within 60 days. The equipment in the hospital is all assigned a priority for completion of preventive maintenance. All life support equipment is listed as urgent. All other equipment that requires regular preventive maintenance is listed as regular. Anything that does not require regular preventive maintenance is listed as deferred. If a work order calls for maintenance on equipment that is being used by a patient, they have to decide whether to temporarily place them on a substitute of that equipment or to come back at a later time when that patient is moved to a different room. Many times, the technicians consult with the nurses on the floor to make this decision. Service Calls When a technician is paged by the office for a service call, they must respond to that page within 10 minutes. From there, it is the department goal to physically respond to the service call within 15 minutes of its receipt. Priority for responding to service calls always goes to life support equipment, but many times it is up to the technician to decide which call is most important. Unable to Locate Equipment During the course of a month, the technicians may receive work orders for equipment they cannot locate. When this occurs, they are required to do a reasonable amount of searching which includes spending the last few days of the month looking for lost equipment. If they are still not able to locate the equipment, they change the status in their computer system to UTL and turn the work order in to their supervisor. The supervisor then turns the UTL work orders into the office and they make note of it, stamp the work order, and return it to the supervisor. He is responsible for keeping it for 120 past the original due date before the equipment goes on the official UTL list. Many times a piece of equipment is found after being placed on the UTL list. If this is the case, they perform the required maintenance and complete the work order. If a piece of equipment has been put on the UTL list twice, it is no longer tracked by clinical engineering. Work Orders There are three possible ways for a technician to accumulate work orders. These include preventive maintenance cycles, service calls, or miscellaneous jobs given by the supervisor. Technicians are expected to fill out and update these work orders with accurate information within a reasonable time of doing work on the equipment. Technicians must be able to account for at least 36 of the 40 hours they work during the week in the work orders. Software In order to track and maintain information about all of the equipment that they are responsible for, the Clinical Engineering department uses software called ISISpro. ISISpro was developed by Aramark with the purpose of tracking medical equipment and providing useful equipment histories, labor tracking, purchasing information, and reports. ("Aramark healthcare: fact,") The most common uses of the software for Clinical Engineering were for work orders. Work orders were printed at the beginning of the month for all equipment that needed preventive maintenance and throughout the month for all equipment that was serviced. Whenever there was a change in the status of the equipment, a new part purchased, or a new problem found in repairing the equipment, the technicians updated ISIS. When the work was completed on a work order, the technician would go into ISIS to complete the work order and provide as much detail as possible to what the problem was with the equipment, any issues faced, and how the problem was resolved. Other relevant information included when completing the work order was the name of the technician that serviced the machine, the date and time of the service, and any parts purchased. The other most useful feature of ISIS was its extensive reporting ability. The system has a large number -3- of pre-written reports that the users can open and run quickly. Users also have the ability to create their own reports based on any fields tracked in the system. The most common reports run by ISIS list the equipment that is due for preventive maintenance and the current UTL list. Any of the information contained in an ISIS report can also be sent to Microsoft Excel which can be useful in communicating with people outside of the department. Overall, ISIS is very complete software that has very few limitations. It is very user friendly which is crucial in a shop of technicians that are not always great with computers and also limits the time needed to train new employees in it. Overall Preventive Maintenance Process This flow chart describes the preventive maintenance process from the very beginning of the month when the preventive maintenance work order is printed out to the filing of a completed preventive maintenance work order. It looks into the process department by department to show how the information flows. Procedures The following flow charts represent the everyday processes performed by the Clinical Engineering technicians: Overall Service Call Process This flow chart describes the service call process from the call to the office to the filing of the completed work order. It gives a look at what each department does and how the information flows from one department to the next. Technician Service Call Process This flow chart describes in greater detail the service call process from the technician’s point of view. It is supplemental to the Overall Service Call Process flow chart. Technician Preventive Maintenance Process This flow chart describes in greater detail the preventive maintenance process from the technician’s point of view. It is supplemental information to the Overall Preventive Maintenance Process flow chart. Work Sampling In order to get a better understanding of where the majority of the technicians’ time was being spent, a work sampling was performed. Because of the nature of the biomedical technician job and the large territory that they cover on any particular day, the work sampling was performed by following one non-service call technician around for a day and making an observation about their activities every five minutes. After three weeks 853 observations were made, thus giving a pretty sound statistic into what a technicians’ time is used for. The following categories were used to describe the observations: -4- Productive Walking Productive walking occurs when the technician is walking to perform work and they have a definite knowledge of where they are headed. Examples of productive walking would be going to pick up a package from shipping and receiving, walking to the Operating Room to talk with one of the supervisors, or returning equipment to the floor after it has been repaired in the shop. Value Added: Yes Locating Equipment Very often towards the end of the month, a technician has a group of work orders that they cannot find the equipment that requires maintenance. In order to locate equipment, technicians usually have to go from floor to floor and department to department to try and locate the equipment. They must make their best attempt to find it somewhere in the hospital before it gets added to the Unable to Locate list. Value Added: No Responding to Page When a technician gets paged from the Clinical Engineering office, they are often informed about a problem that they need to address. Anytime the technician was on the phone finding out this information from the office it was classified as responding to page. Value Added: No Maintaining Equipment Maintaining Equipment is the category used to describe any time a technician physically had their hands on a machine to work on it. Maintaining equipment could apply to preventive maintenance, repairs, inspections, or setting up equipment. Value Added: Yes Personal Break This category was used anytime the employee was using the restroom or if they had any downtime. Value Added: No Filling out Work Orders When a technician is finished working on a piece of equipment, the work order must be updated. This applies to regular preventive maintenance as well as unexpected repairs. Filling out work orders involves the physical action of filling out work orders as well as writing down the essential information for a work order that they may not have access to at the time. Value Added: Yes Helping Other Technicians Many times a technician would come across a problem that they needed some assistance in solving. This could be because they needed someone else’s perspective on the problem or because they just did not have the experience on a certain machine to know what the problem was. In this case, the other technicians were very helpful and provided assistance in any way they could. Value Added: Yes/No Typing Work Orders/P.O.’s When a technician is looking up a work order, checking on the status of a work order, completing a work order, or writing a purchase order it goes in this category. Technicians spend a large part of their day on the computer filling out paperwork for changes in a piece of equipment’s status, updating ISIS, and writing purchase orders. Value Added: Yes Waiting Whenever the technician had to briefly wait on someone to do something, it was put in this category. Value Added: No Productive Talking Productive talking occurs any time the technician is speaking with another person about job related issues. Some examples of this would be talking to their supervisor, discussing how to fix a piece of equipment with another technician, instructing an outside vendor on where to find equipment, and updating floor supervisors about work done on their equipment. Value Added: Yes/No Unproductive Talking Unproductive talking occurs when the technician is talking with someone else about non work related issues. Value Added: No Looking up Equipment History If there was a discrepancy between paperwork or if there was a question about the last time a piece of equipment was repaired, the tech either looked up the equipment history themselves or called the office to have them look it up. Value Added: No Checking Email The technicians usually checked their email first thing in the morning and very rarely accessed it again during the day. Value Added: Yes/No Unproductive Phone Call This category was used for any non work related phone conversation. Value Added: No -5- Accessing Equipment On rare occasions the technicians had to empty out closets or move other equipment to access something that needed maintenance. Value Added: No Observation Sheet A sheet with the following format was used to record observations of the technicians’ activities in a day. Activities 1 2 3 4 5 6 7 8 9 10 Productive Walking Productive Phone Call A productive phone call occurred when the technicians were either giving or receiving important work related information. It is different from “Responding to Page” in that a productive phone call was not a request to go to a certain floor to perform service. Some examples of productive phone calls included calling a vendor to schedule maintenance, calling a company about billing questions, and calling a floor supervisor to update them on the status of their equipment. Value Added: Yes/No Locating equipment Filling out Work Order Info Typing Work Orders Productive Talking Unproductive Talking Responding to Page Maintaining Equipment Personal Break Helping Other Techs Waiting Looking up equipment history Checking email Unproductive phone call Accessing equipment Productive Phone Picking up Broken Equipment Whenever a technician had to take a piece of equipment back to the shop for repair it went in this category. Value Added: Yes Ordering Parts This category covered everything involved with ordering parts from physically talking on the phone with the vendor to looking up a part online. Value Added: Yes Picking up Broken Equipment Ordering Parts Other Productive Locating Parts in Shop *Observations Made Every 5 Minutes Notes: Results The following are the results of the work sampling: Results Other Productive Any work related tasks not covered by one of the other categories went here. Value Added: Yes/No Locating Parts in Shop Sometimes the technician had to try and find a part to fix a piece of equipment or find a misplaced piece of equipment. Anytime they had to locate a part or equipment before using it, it went in this category. Value Added: No Observations % of Time Productive Walking 98 11% Locating equipment 41 5% Filling out Work Order Info 12 1% Typing Work Orders/P.O.'s 100 12% Productive Talking 83 10% Unproductive Talking 7 1% Responding to Page 24 3% Maintaining Equipment 247 29% Personal Break 4 0% Helping Other Techs 23 3% Waiting 10 1% Looking up equipment history 7 1% Checking email 19 2% Unproductive phone call 2 0% Accessing equipment 1 0% Productive Phone 39 5% Picking up Broken Equipment 11 1% Ordering Parts 29 3% Other Productive 86 10% Locating Parts in Shop 10 1% Total Observations 853 -6- Percent of Time Spent on Activities real sense of pride about their job and putting the patients’ needs first. Productive Talking 10% Locating equipment 5% PM Analysis Maintaining Equipment 28% Productive Walking 11% Productive Phone 5% Typing Work Orders/P.O.'s 12% Unproductive Activity 2% Other Productive 27% Analysis of Results Looking at the results, there are a few activities that have different percentages than expected. Maintaining equipment is surprisingly low at 28% since the purpose of the Clinical Engineering department is to keep the equipment maintained. However, productive walking, typing work orders and purchase orders, and productive talking are surprisingly high. Unfortunately during observations, it did not seem as though any of these areas have any real potential for improvement. Productive walking is always going to be a large portion of the employees’ time in a medical center the size of Mount Sinai. Since the department is located on the ninth floor which can only be accessed by one elevator that is also used for a large amount of patient transportation, most trips take the employee a minimum of five minutes of travel time. Typing work orders and purchase orders seems especially high as well, but there is no real way to decrease the amount of paperwork that has to be done. Almost all of the paperwork the technicians do is required by the Joint Commission and must be completed for the department to remain compliant. Productive talking will always be a large portion of time as well since the technicians must update their supervisor, floor supervisors, technicians, and outside service vendors on changes in equipment status as well as get updates on what work needs to be performed on equipment. The encouraging statistic that came from this work sampling is the small percentage of time spent on unproductive activities. The hospital can feel confident that the technicians were working hard at all times to get the equipment functioning properly in the fastest way possible. Another encouraging observation was that if a technician happened to come across a piece of equipment that was being used, but did not look right, they stopped what they were doing and fixed it on the spot. The staff of the Clinical Engineering department did seem to have a The following information came from a report run in ISIS. This information shows the number of preventive maintenance work orders by status and priority from January 1, 2009 through December 31, 2009. A cancelled work order occurs after a piece of equipment is on its second UTL or the department does not want the equipment anymore. Remove from service is the work order issued to remove the equipment from the active assets in the system. The numbers show that the department is very reliable when it comes to finishing their work orders on time. Only two percent of the routine work orders were completed after their due dates. This is most likely caused by the technicians not being able to locate a piece of equipment until after its due date. The rest of the equipment however was completed exactly on time. Cancelled Urgent Routine Deferred Completed Urgent Completed w/in 24 hours Completed w/in 30 days Routine Completed w/in 5-8 hours Completed w/in 24 hours Completed w/in 30 days Completed w/in 60 days Completed w/in 90 days Completion time exceeds 90 days Deferred Completed w/in No specified priority Completed w/in Completed w/in Completed w/in Completed w/in Completed w/in Remove From Service Routine Unable to Locate Routine No specified priority 30 days 2 hours 2-4 hours 5-8 hours 24 hours 30 days Total Year 539 28 507 4 4177 309 4 305 3753 12 24 3632 18 12 57 8 8 105 50 1 5 40 9 49 49 83 82 1 Percentage 11% 1% 10% 0% 86% 6% 0% 6% 77% 0% 0% 75% 0% 0% 1% 0% 0% 2% 1% 0% 0% 1% 0% 1% 1% 2% 2% 0% 4848 Completed On Time Urgent 100% Routine 98% Deferred 100% Not Specified 100% Challenges Faced Locating Equipment The biggest challenge by far for the Clinical Engineering department in meeting their goal is locating equipment on the hospital floors. All equipment tracked by the department has its assigned location stored in their computer system, however many times the equipment moves and the department is not notified. When the time comes to perform preventive maintenance on this -7- equipment, the technician has to spend time at the end of the month walking from floor to floor in the hospital checking in every room trying to locate the equipment. They must give their best possible effort to find the equipment to make sure it does not get used without first getting its preventive maintenance done. Locating the equipment can waste a whole day of a technician’s time that could be spent working on other equipment. Equipment Abuse Much of the time, especially in the Imaging Department of Clinical Engineering, the repairs that are needed on equipment are caused by abuse. This abuse is not intentional, but people sometimes get careless with the equipment and damages arise out of their carelessness. Shown below are two pictures that display examples of equipment misuse provided by the Imaging department supervisor. Picture 1 shows an OEC Uroview 2600 table underside that was damaged when a table with a patient on it was lowered onto another piece of equipment during a procedure, thus creating a large dent in the metal. Picture 2 is an example of an ultrasound probe that was forced into its system with Picture 1 the locks closed instead of open. Five probes were found in this condition with three of them resulting in a $300 cost to the hospital Picture 2 each. The other two have not yet been replaced or repaired because the cost was estimated to be around $4,500 each. Simple moments of carelessness can have a huge impact on the cost of equipment maintenance for the hospital as it can take a long time for the Clinical Engineering staff to fix the machinery as well as cost a large amount of money for new parts. Staffing As previously mentioned the staffing issues Clinical Engineering has faced have been a difficult challenge to overcome. The constant fluctuation of employee numbers as well as having to familiarize new employees with their new setting not only creates stress on the employees, but makes it harder for them to work on the equipment in need of repair. Recommendations Improve Equipment Tracking The biggest challenge that the Clinical Engineering department consistently faces in performing their job is finding equipment. Many times there is equipment that is given out by Central Services that could be located anywhere in the hospital and it is constantly moving. When a technician has to try and locate that piece of equipment, they have to repeatedly check rooms because of the possibility that it got reassigned since the last time they looked for it. When technicians cannot locate equipment, it creates problems in that the equipment does not get serviced on time or it is not able to be found at all. Equipment that is not serviced on time will most likely still be used by hospital employees and is a liability to the hospital if something were to happen to a patient after use. The ideal situation would be if the individual floors had a method of tracking the rooms that their larger equipment is assigned to and where their smaller equipment is stored. This way Clinical Engineering could have a window on their computer system that allowed them to look up a piece of equipment and find out which room it was in. However, this solution is not only very expensive, but it would also be hard to maintain. The nursing staff is already very busy helping patients and this additional tracking would most likely not happen. Instead, the most feasible method for improving equipment tracking would be just to focus on the current system Central Services uses to track their equipment. Clinical Engineering could be provided a window into the Central Services system that would allow them to see what room a particular piece of equipment is located in. The only thing that they would need to provide is a serial number and Aramark identification number for all of the equipment distributed by Central Services which could easily be provided through ISIS. Due to the limited amount of equipment distributed by Central Services, making this change would not make a dramatic change in the amount of equipment on the UTL list or the amount of time spent locating equipment, but it would help. This change would be relatively simple and would not involve any extra work by Central Services. -8- Eventually the system could be expanded to include all of the equipment in the hospital. Currently Ricardo Abella from Project Management and Duran Whilhite from Purchasing are working on setting up a database with a listing of all of the equipment the hospital owns, and what floor it is located on. If this database remains updated when equipment moves from floor to floor, giving Clinical Engineering a window to view this information would once again be helpful to at least narrow down the search area for an individual piece of equipment. Once again, all that Clinical Engineering would need to do is provide a spreadsheet with the Aramark identification number and the serial number and the database would update itself. Then when they needed to locate a piece of equipment, they would type in the I.D. number and be able to see what floor the equipment is assigned to. A database that requires the floors to update equipment moves would be far more reliable making Clinical Engineering track the location because currently, the floors rarely communicate with Clinical Engineering when equipment moves. Instead, that information is updated whenever a work order is issued for a machine and the technician finds it in a different location than is listed. Locating equipment is always going to be an issue faced by any Clinical Engineering department, but providing them with as much information as possible about the location will help improve their reliability. Improved reliability means improved patient safety by preventing the use of out-of-date equipment. More Detailed Work Order Status Information It would be helpful for going back and looking at the response times to service calls if the technicians were more detailed in reporting the times on a work order. Currently the times that are recorded are the time a technician opens a work order, the times when the technician updates the status of the work order, and the time the technician closes the work order. Ideally, the time a call came in, the time the technician responded to the caller, and the time the equipment was fixed would be tracked in order to build statistics about response times. This would give the department a better idea of whether they are reaching their goals or not. This added detail would be very helpful and be a limited amount of additional work. Establish a Capital Expense Committee One idea that the Imaging department supervisor repeatedly brought up during my time with him was the idea of having a Capital Expense Committee. This committee would consist of employees from multiple departments and would be responsible for making decisions on the higher priced medical equipment. Having people from the different departments would be beneficial because it would provide one meeting place for people with different expertise’s to discuss a purchase that is a major expense to the hospital. Insight from the different employees could prove to be very valuable because new ideas that wouldn’t normally be thought about could come up. Having large equipment purchases go through a Capital Expense Committee seems like a logical step so the hospital gets the equipment it actually needs and gets the most out of the money spent. Conclusion Overall, it appears that the Clinical Engineering department at Mount Sinai Medical Center is very reliable in their work and open to any possible changes for the better. After reviewing the department for six weeks and getting an in depth look at their operations, I feel that the only significant improvements that can be made are in improving the equipment tracking in the hospital, getting more detailed status information on work orders, and the creation of a Capital Expense Committee. Other than these three recommendations, it seems that the department is very thorough in their work and should continue to operate with their current methods. Acknowledgements Special thanks to Ben Davis and Angel Palin for giving me an opportunity to work and Mount Sinai and gain valuable experience. Thanks to Tamara Ali and Perry Fontanilla for providing assistance and guidance on the project. Thanks to Dr. Nina Miville for helping set up my internship opportunity and providing invaluable guidance to the University of Miami chapter of the Institute of Industrial Engineers. References 1) About aramark. (n.d.). Retrieved from http://www.aramark.com/aboutaramark/ 2) Aramark healthcare: fact sheets. (n.d.). Retrieved from http://www.aramarkhealthcare.com/UtilityDetail. aspx?PostingID=705&ChannelID=343 About the Author Christopher Maloney is a senior in Industrial Engineering at the University of Miami who will be pursuing a graduate degree starting in January of 2011. He is currently involved as the webmaster with the University of Miami chapter of Institute of Industrial Engineers and as the treasurer for the National Society of Black Engineers. This paper was written during his time as a Hospital Administrative Fellow intern at Mount Sinai Medical Center in Miami Beach, FL as a project to review the activities of the Clinical Engineering Department. In addition to Mount Sinai, he did an internship with Dueco, Inc. in Waukesha, WI. -9-