Reducing Blood Draws In Critically Ill Patients
advertisement

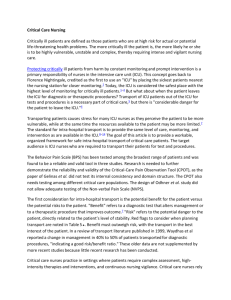
PROJECT NAME: Reducing Blood Draws In Critically Ill Patients Institution: The University of Texas M.D. Anderson Cancer Center Primary Author: Melissa McLenon, DNP, APRN, ACNP-BC Secondary Author: Gregory Botz, MD Course Participants: Natalie Clanton, RN, CCRN, Latoi Tatum, MHA, Blake Brookshire, MD Project Category: Efficiency Overview Several studies have shown that diagnostic laboratory testing is a significant contributor to anemia in critically ill patients. Phlebotomy practices also contribute to the frequency of red blood cell transfusions, and research has proven the transfusion of blood products is associated with higher mortality and longer intensive care unit (ICU) length of stay. We recognized the need to decrease the frequency of blood draws among critically ill patients in our ICU. Our team collected 4 weeks of baseline data to determine the frequency and volume of blood draws per 24 hours, per critically ill patient (figure 1)in a 10 bed medical ICU pod. We enlisted key stakeholders, including members of the multidisciplinary ICU team, the clinical laboratory, information technology, and administrative staff to determine the factors associated with the high frequency of blood draws. Through the alignment of our goal with the institutional goals, we strived to improve operating efficiency, both at the departmental and institutional level. Aim Statement To reduce the frequency of blood draw events, per 24 hours, per critically ill patient, by 20% by June 10, 2012. Measures of Success Pre-intervention data was collected for 4 weeks, including the volume and frequency of blood draw events on each patient in a 10 bed medical ICU pod. We also collected data on the number of lab tests ordered as well as the number of ordering providers. We then collected an additional 3 months of data. The goal was to reduce the frequency of blood draw events per ICU patient per 24 hours by 20%. Use of Quality Tools We used a brainstorming session with key stakeholders to identify factors that were important to blood draws in the ICU. We then created an affinity diagram to consolidate ideas which became the elements of our Ishikawa diagram (figure 2). Next, we developed a process chart (figure 3) to determine where potential interventions may have the greatest impact. Once data was being collected, we generated run charts (figure 4, 5) to reflect the data over time. Interventions To focus on potential interventions, the ICU staff completed a survey on their perceptions about blood draws in the ICU, and provided feedback on efforts to minimize blood draws in critically ill patients. The most common factor identified in excessive blood draws was related to inadequate communication. Therefore, our primary intervention was aimed at improving communication about lab testing and blood draw frequency among the healthcare team. We added a lab testing and blood draw item to our ICU daily rounding checklist to focus a multidisciplinary discussion among the ICU team. We also formalized a discussion between the licensed laboratory technicians (LLTs) to reduce the redundancy of ordered tests and frequency of one-off blood draw events, and to reduce scheduled blood draws during blood products or electrolyte administration (figure 6). This increased the ICU nurse and LLT autonomy to reschedule non-emergent blood draws until blood products and electrolyte replacements were completed. We also formalized a process to allow non-emergent interval lab tests to be clustered with the next scheduled lab draw event, unless specifically needed at that time. In addition, the baseline data were shown to the ICU physicians and midlevel providers (MLP) during staff meetings as an education strategy. Discussion included attention to provider variation in lab ordering practices, lab testing redundancy, serial labs order frequency and duration, and laboratory order set utilization. This was followed by additional brainstorming on our current practices and the potential impact on our patients. Results Baseline data showed a wide practice variation among providers. The number of blood draw events ranged from 2-14 per patient per 24 hours, with an average of 3.99 per patient. Post implementation, the number of blood draw events ranged from 0-12 and the average number of blood draws per patient per 24 hours decreased to 2.97. Pre-intervention, blood volume collected with each blood draw event ranged from 6cc to 250cc per patient per 24 hours, with an average of 46.79cc per patient. Post implementation, the volume of blood collected with each blood draw ranged from 0165cc, with an average of 36.84cc per patient per 24 hours. Overall, there was a 25% reduction in the number of blood draws and a 21% reduction in the volume of blood drawn with each blood draw following the interventions. Also, the median and mode of the two variables decreased over the 3 month post-implementation period. Revenue Enhancement /Cost Avoidance / Generalizability The return on investment for this project is multifaceted. It is difficult to assign costs to blood draw events due to our current charge system. This has made us aware of another opportunity for improvement as this project moves forward. The charge for our routine laboratory tests (chemistry panel, complete blood count, arterial blood gas) is estimated at $620. That does not include the personnel and equipment that is necessary to complete the testing. Another potential cost savings associated with a decrease in the volume of blood draws is a decrease in the frequency of blood transfusions. The average ICU length of stay (LOS) is 5 days. However, the LOS varies from days to months in the medical ICU. By reducing the daily frequency and volume of blood draws, there will be a decrease in the degree of anemia associated with the blood draws. Ultimately, this will result in a decrease in the number of blood transfusions, as well as the costs and complications associated with blood transfusions. The charge for an uncomplicated unit of packed red blood cells is approximately $1400. However, that does not include the preparation nor the monitoring required to transfuse the blood. Nor does this charge account for complicated transfusions, pre-medications, or transfusion reactions. Several studies have shown complications associated with blood transfusions include an increase in ICU LOS, mortality, and ventilator days, transfusion related acute lung injury, and other adverse reactions. Another potential cost savings associated with a decrease in the frequency of blood draws is a decrease in the incidence of central line associated blood stream infections (CLABSI). Because most of our critically ill oncological patients have central venous catheters, the blood is drawn from these catheters or arterial catheters. Each time these lines are accessed for a blood draw, there is a risk of contamination and line infection. The cost associated with a CLABSI is estimated at $14,000 per critically ill patient. Due to the potential complications associated with excessive blood draws, decreasing the frequency potentially results in improved ICU throughput. This will allow for more timely transfer of patients out of the ICU to provide access and availability for critically ill patients who require ICU services. Reducing the frequency of blood draws results in quality outcomes as well as clinical and financial outcomes. Patient and provider satisfaction is difficult to measure in terms of cost, but the quality of care is greatly improved. Our patients have the right to care that is safe, efficient, equitable, effective, timely, and patient centered. Conclusions and Next Steps Studies have shown that excessive blood draws in the ICU results in increased mortality, LOS, and need for blood transfusions. Our team identified that our patients were experiencing frequent blood draws and redundant laboratory testing, mostly related to a lack of communication among the ICU multidisciplinary team. Our interventions to reduce the frequency and volume of blood draws per critically ill patient per day were successful. We want to expand the scope of our project to include critically ill surgical patients, who will also benefit from a reduction in the frequency of laboratory testing. The surgical teams will be included in this process. We will also focus our attention on other factors identified in the process map and Ishikawa diagram which contributes to the frequency and redundancy of laboratory testing. Another goal is to meet with representatives from information technology and laboratory medicine to evaluate methods of order entry modification in an effort to cluster lab orders, alert notifications for redundant labs, automatic discontinuation of serial labs at 24 hours, and other technology issues that may be modifiable. Also, we will evaluate alternates to improve our charge system in an effort for departments to receive feedback on the costs associated with the laboratory testing. We hope to see our efforts to minimize the frequency and volume of blood draws and laboratory testing spread throughout the institution. We will continue to reinforce our education and training and seek support from departmental and institutional leadership. Data Collection Tools 6am-12pm 12pm-6pm 6pm-12am 12am-6am Number of vials Bed 1 cc of blood Number of draws Number of vials Bed 2 cc of blood Number of draws Number of vials Bed 3 cc of blood Number of draws Number of vials Bed 4 cc of blood Number of draws Figure 1: Data collection tool Ishikawa Diagram Errors System Equipment lack of blood conserving system 2 different systems clotted blood delay in stat orders lost labs lack of pedi tubes inability for add-ons lack of computer prompts order entry error unable to view redundant labs scheduled serial labs acuity order set Process read only access unaware of scheduled labs nurses/RT lack of communication lack of awareness . different providers ordering labs tube system heirarchial issues provider preferences People Figure 2: Ishikawa (cause and effect) diagram Problem Statement Excess volume and frequency of lab draws among critically ill patients. order is placed in Clinic Station Multiple providers ordering labs without discussion Order is placed in que for PSC PSC acknowledges order for labs Process for Lab Ordering Request for lab is generated in clinic station STAT lab? No Request processed from Clinic station to Cerner (approx. 15 min) Lab requisition generated Yes System does not automatically time with other scheduled labs No coordination of timing w/other scheduled labs ICU team reviews lab results Results are placed in Clinic station No Critical results Lab is processed Page LLT to draw lab Lab is received and logged into system Multiple labs on multiple patients sent to lab via pneumatic tube system Yes Lab calls ICU team Lack of available tubes No Action needed Yes Intervention Monitor patient Figure 3: Process Map Affect on Patient LLT draws lab No contact with RN prior to drawing labs 70 Pre-intervention MEAN = 3.99 Pre-intervention MEAN = 46.79 5/14 5/15 5/16 5/17 5/18 5/19 5/20 5/21 5/22 5/23 5/24 5/25 5/26 5/27 5/28 5/29 5/30 5/31 6/1 6/2 6/3 6/4 6/5 6/6 6/7 6/8 6/9 6/10 2/13 2/14 2/15 2/16 2/17 2/18 2/19 2/20 2/21 2/22 2/23 2/24 2/25 2/26 2/27 2/28 2/29 3/1 3/2 3/3 3/4 3/5 3/6 3/7 3/8 3/9 3/10 3/11 Frequency of Draws (per pt per day) 7 5/14 5/15 5/16 5/17 5/18 5/19 5/20 5/21 5/22 5/23 5/24 5/25 5/26 5/27 5/28 5/29 5/30 5/31 6/1 6/2 6/3 6/4 6/5 6/6 6/7 6/8 6/9 6/10 2/13 2/14 2/15 2/16 2/17 2/18 2/19 2/20 2/21 2/22 2/23 2/24 2/25 2/26 2/27 2/28 2/29 3/1 3/2 3/3 3/4 3/5 3/6 3/7 3/8 3/9 3/10 3/11 ml of Blood Drawn (per pt per day) Average Frequency of ICU Blood Draws 6.5 Post-Intervention MEAN = 2.97 5.5 6 5 4.5 4 3.5 3 2.5 2 1.5 1 0.5 0 Figure 4: Frequency of blood draws pre- and post-intervention Average Daily Volume of Blood Draws Post- intervention MEAN = 36.84 60 50 40 30 20 10 0 Figure 5: Daily volume of blood pre- and post-intervention Process for Lab Ordering order is placed in Clinic Station Multiple providers ordering labs without discussion Order is placed in que for PSC PSC acknowledges order for labs Request for lab is generated in clinic station System does not automatically time with other scheduled labs No coordination of timing w/other scheduled labs ICU team reviews lab results Results are placed in Clinic station No Critical results Lab is processed STAT lab? No Request processed from Clinic station to Cerner (approx. 15 min) Yes Page LLT to draw lab Lab is received and logged into system Multiple labs on multiple patients sent to lab via pneumatic tube system Yes Lab calls ICU team Lack of available tubes No Action needed Yes Intervention Monitor patient Affect on Patient Figure 6: Process map post-intervention Lab requisition generated Interventions LLT draws lab No contact with RN prior to drawing labs