Saving 1000 lives publication
advertisement

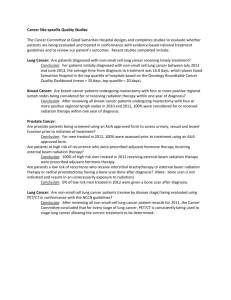
Saving 1000 Lives Improving Outcomes: A Strategy for Earlier Diagnosis of Cancer in London Commissioning guidance for London PCT clusters March 2012 Strategy for Increasing Early Diagnosis in London Foreword The Model of Care for Cancer Services in London (CSL August 2010) gives recommendations for implementation that would most certainly contribute to improving survival rates to meet the best in Europe and could translate into saving 1,000 Londoners’ lives annually. This is reflected in Improving Outcomes: A Strategy for Cancer (IOSC, DH January 2011) which commits to the challenge of saving 5,000 lives from cancer in England, every year, by 2014/15. It summarises the actions that are needed in 4 categories: those that reduce the incidence of preventable cancer through lifestyle changes, those that improve access to screening services where there is evidence that this will save lives those that will achieve earlier diagnosis those that will ensure that all patients have access to the best possible treatment. Within this framework, it states that; ‘diagnosis of cancer at a later stage is generally agreed to be the single most important reason for the lower survival rates in England’. The aim of this strategy is to improve survival from cancer for Londoners through ensuring that cancer is diagnosed earlier. Achieving this will lead to the saving of lives set out in the model of care and will be measured initially by one year survival rates (a proxy measure for later stage at diagnosis) and, in due course, by improved five year survival. Studies comparing five year survival in England to the best in Europe have shown that much of the difference in survival occurs in the first year following diagnosis - highlighting the importance of earlier diagnosis. The image shown on the front cover of this document is from the Office of National Statistics (ONS) 2010. It shows 1 year survival from all cancers in 2006 and illustrates clearly that inequalities exist across London. Out of 100 people with cancer from the areas shaded in lighter yellow, 5 more will die within a year of diagnosis than those from the darker blue areas. At the same time all of London lags behind the best in Europe – our task is to take actions that paint all of London a uniform and darker blue! Given the number of lives that are there to be saved – deaths that can be avoided – there are no more important or urgent actions than those proposed to be commissioned in this document. Both the model of care and the IOSC set out the key elements of the early detection pathway that are integral to the National Awareness and Early Detection Initiative (NAEDI). To improve earlier detection and diagnosis in London we need to: increase public awareness of cancer signs and symptoms overcome barriers to presentation to primary care overcome clinical and system barriers to prompt onward referral within and between primary and secondary care improve GP access to diagnostic tests to help confirm or exclude a diagnosis of cancer ensure that, once cancer is suspected, there is improved access to specialist pathways in secondary care and that the same guidelines are applied to patients who present to hospitals through non-urgent or emergency care pathways. This document recommends priority actions for a systematic spread of the most effective interventions for earlier detection across all of London. The very nature of London with its existing health inequalities and socio-economic diversity means that this pan-London approach needs be matched by integrated action at Health and Well Being Board and CCG levels. Understanding gained from local needs assessments should inform actions to ensure that they are effective across the whole population. Without this, there is a risk of widening inequalities. Existing and emerging network/cluster and borough level strategies and actions must be supported, strengthened, and integrated with this London strategy to ensure that inequalities are tackled. The proposed priorities are based on national commissioning guidance and represent accepted best practice. It is necessary for there to be a whole London and whole systems approach involving all stakeholders as a key objective. We have an important opportunity, through this strategy, to enable and support clinicians to respond to the individual needs of their patients, by referring on through evidence-based pathways. This opportunity is enhanced by the announcement that the prevention and earlier detection of cancer will be one of three key workstreams of the Mayor’s London Health Improvement Board (LHIB). It is essential that the commissioning guidance herein should integrate with the Proposals for Action of the LHIB workstream. The implementation plan included in this document should respond to and coordinate with those of the LHIB workstream and programme management of implementation should be integrated wherever possible. There are well understood approaches for cost-effective action and, without the coordinated commissioning and whole systems implementation of these actions, we will not reach the projected saving of lives. The section below on screening highlights that, following a programme of targeted interventions, for example, the uptake of breast screening in inner East London has improved very significantly. Uptake now approaches the national minimum standard and is an important illustration that the behaviour of people in deprived and diverse communities is amenable to focussed action. Dr Tony Brzezicki Chair Public Health and Primary Care Sub Group of the London Cancer Review Contents Foreword Executive summary and recommendations 5 1. Background 8 2 London Health Improvement Board 9 3. Aims and Objectives 9 4. Baseline 10 4.1 Survival 10 4.2 Stage at presentation 10 4.3 Co-morbidity 10 4.4 Screening 11 4.5 Population awareness 11 4.6 GP referrals 11 Priorities for London 12 Information and intelligence 13 Public awareness 14 GP engagement 14 Access to diagnostics 14 Integrated Cancer System 15 6. Resources 16 7. Commissioning support tools 17 8. Implementation plan 18 Appendix 1. Potential lives saved 20 Appendix 2. Incidence of breast colorectal and lung cancer rates in London boroughs 21 Appendix 3. Survival from breast colorectal and lung cancers in London boroughs 22 5. Executive Summary Early detection and treatment for cancer is critical for survival; for example 90% of women diagnosed with breast cancer at stage 1 will survive at least 5 years, whilst 90% of those diagnosed at stage 4 will have died before 5 years. Early detection has therefore become the key government strategy for improving cancer. It is estimated that 11,000 lives could be saved nationally if survival rates in England were the same as the best in Europe. This corresponds to saving, by 2014/15, 1,000 lives in London per year, every year. London has survival rates for cancer that are some of the best and the worst in the country. Research and analysis about stage at presentation and co-morbidities is needed to inform our understanding and should be required from all Trusts. Local and national surveys have shown that awareness of cancer symptoms is poor in general and is worse in men, lower socio-economic groups and BME groups. These surveys also show that many people perceive barriers that prevent them going to their GP. Although screening is not formally within the scope of this strategy, cancer screening programmes make a significant contribution to early diagnosis. Uptake of all screening programmes is poorer in London than the national average with rates particularly low in Inner London PCTs. Nevertheless, there have been encouraging improvements over the last year in a number of PCTs. It is key that implementation of this strategy and those for cancer screening, led by the London Screening Improvement Board, are closely linked and that commissioning arrangements are aligned. This will include the potential impact on the bowel screening programme of the national bowel cancer awareness campaign. Although there has existed a fast track pathway for suspected cancer patients for 10 years, less than half of patients with cancer are referred via this pathway; a quarter of cancer patients first present at A&E. Many PCTs across London have developed training and audit programmes to support GPs to improve referrals. Comprehensive programmes need to be developed to further support primary care practitioners in early diagnosis. Cancer networks and PCTs, working with public health and primary care colleagues, have implemented a number of early detection initiatives, many funded with Department of Health or National Cancer Action Team (NCAT) funds. These initiatives now need to be developed into a sustainable programme of work across London to address the following key areas: increase public awareness of cancer signs and symptoms overcome barriers to presentation to primary care improve GP access to diagnostic tests to help them to confirm or exclude a diagnosis of cancer overcome clinical and system barriers to prompt onward referral within and between primary and secondary care. A number of actions have been identified and prioritised to help improve early diagnosis across London. These are set out below in the order of the patient pathway: It is recommended that: A pan London, high quality, cancer intelligence service should be configured, through the coordination and focusing of existing resources and expertise, to ensure that implementation is based on assessment of needs and effectiveness, and that the impact of actions are monitored and evaluated. This will integrate with, be part of and not separate from, overall intelligence functions as they emerge from the transition to the new NHS commissioning system and including Public Health England. Beginning with the National Bowel Cancer Symptoms Awareness Campaign, measures that improve both the public awareness of symptoms of cancer and encourage early presentation to primary care and, where appropriate, improve uptake of screening services must be commissioned and implemented. This will best be achieved by the configuration of a small specialist team at a London level in coordination with action and ‘advocacy’ at a local level. Primary care leadership is essential to the whole of the early detection pathway. It is recommended that each CCG should identify a Primary Care Cancer Lead (PCCL) resourced with a minimum of one and up to 2 sessions per week who should be supported by robust cancer network level leadership sustainably resourced in line with national guidance. Primary Care leadership will have an important role in ensuring that GPs have up to date knowledge of cancer guidelines for referral and diagnosis. Commissioners should ensure that all GPs in London have direct access to the four diagnostic tests identified by Improving Outcomes: A Strategy for Cancer and should request tests in line with the guidance and pathways to be issued by the Department of Health. Primary care should ensure that access to these tests following patient presentation is rapid. In addition, providers should ensure that results and reports are available within two weeks and that abnormal findings result in the direct referral into specialist pathways. In alignment with NICE guidance, there needs to be information and support available for those with raised familial risks of cancer so that they access primary care and, where appropriate, screening services, as early as possible. The output specifications of the commissioned pathways of Integrated Cancer Systems (ICS) should include measures for improved one year survival, as a proxy for longer term survival, and stage at presentation and emergency presentation proxies for one year survival. ICSs should work closely with primary care, CCGs and networks across the whole of the early detection pathway but with a particular emphasis on optimising referral from primary care. They must ensure ongoing prompt access to specialist enhanced pathways once cancer is suspected and the Acute Oncology Services should provide an enhanced pathway for those who continue to present as emergencies. The cost of cancer in England, including both direct NHS costs and societal costs such as the loss of productivity, has been estimated at approximately £18 billion per annum (Featherstone and Whitham, Policy Exchange 2010). The same source proposes that if UK survival rates improve to the best in Europe then a substantial reduction in cost will result, £10 billion cumulatively by 2020. These economic benefits will be available to, and important for, London and Londoners. The DH financial impact assessment of the NAEDI strategy, published in January 2011, sets out detailed cost modelling and analysis of the impact of earlier diagnosis, on five different cancers. There is potential for increases in diagnostic costs partially offset by a reduction in treatment costs and it is also recognised that there are timing effects as elements of the diagnostic costs are brought forward to an earlier period. Their overall conclusion is that earlier detection would represent value for money but would not be cost saving. This is consistent with the conclusion reached in the model of care. There are difficulties and variability in estimating these effects. The DH work was based on national statistics; the impact on London needs to be better understood as there are differences from the national picture, for example the lower levels of screening uptake. The financial impact will also depend on the speed at which implementation, including for screening, is planned and delivered. The next stage of analysis will be take the model used by the DH and use data and assumptions that are appropriate for the capital so that the overall financial impact can be included in a business case. It is recommended that commissioners should: Allow for an expected increase in use of diagnostic and treatment costs in risk reserves for 2012-13 until detailed plans are developed Include provision in commissioning strategy plans for awareness campaigning at the level of £100,000 per 200,000 population, Pick up the current non-recurring DH/NCAT funding of network GP leadership allowing £150,000 for London-wide GP leadership and, in addition, CCGs should budget for PCCL posts at 1 or 2 sessions per week per CCG. The best practice pathways being developed as the basis of contracts with the ICSs for cancer care will reflect base practice to support earlier diagnosis. Commissioners and trusts will need to work closely to model capacity and activity in key diagnostic areas. Commissioners will also need to ensure that provision is made for ongoing programmes to improve population awareness. Although some programmes may be centrally or regionally funded, the success of awareness programme in improving early diagnosis will also depend on local responses in primary care. The LHIB early diagnosis campaigns will have an important contribution to make to this work. Health services will need to work closely with local government to make sure that strategies and plans are joined up. Harnessing the power of the voluntary sector to support these programmes will greatly enhance the potential impact. There is a need to move away from short term, project based work to embedding organisational and cultural changes in the delivery of health and other services to ensure a sustained and ongoing engagement of patients and staff in early cancer detection. It is important to acknowledge that the delivery model for earlier detection is complex and this is particularly the case as the NHS moves to the new commissioning arrangements and, for London, the Integrated Cancer Systems develop. Implementation plans will require further development as changes emerge, and to ensure clarity on leadership and responsibility and accountability for actions. Recommendation: The implementation plan included in this document should be developed and taken forward at London level and be aligned with the London Health Improvement workstream and with the full range of NHS structures in transition to the new commissioning arrangements 1. Background In general, the earlier a cancer can be diagnosed the greater the prospect of survival. The National Cancer Director has often illustrated this with breast cancer: If breast cancer is diagnosed early at ‘Stage 1’ then 90% of patients will survive beyond 5 years whereas if diagnosed late at ‘Stage 4’ then 90% will die within 5 years. In Improving Outcomes - a Strategy for Cancer, the Government made a commitment to bring England's cancer survival rates up to the European average by 2014/15. This would be equivalent to saving roughly 5,000 additional lives per year in England. The model of care for London identified that around 1,000 lives a year are lost in London when compared to the best in Europe. Studies comparing five year survival in England to the best in Europe have shown that much of the difference occurs in the first year following diagnosis. The majority of these avoidable deaths are likely to be due to late diagnosis. We now need to attain the overall objective for London to save lives by detecting and diagnosing cancer as early as possible. The National Awareness and Early Detection Initiative (NAEDI), the public sector/third sector partnership between the Department of Health, the National Cancer Action Team (NCAT) and Cancer Research UK set out three key workstreams for commissioning. Increase public awareness of cancer signs and symptoms, and consequent presentation to primary care. Facilitate onward clinical referral within and between primary and secondary care. Improve GP access to diagnostic tests to help them to confirm or exclude a diagnosis of cancer. Cancer networks, working with PCTs, public health, primary care and the full range of stakeholders, have led significant progress in implementing local awareness and early detection initiatives. Whilst some PCTs have prioritised significant investment, many of these initiatives have been funded by the Department of Health and the NCAT through competitive bidding processes. This strategy, through the London Cancer Commissioning Intentions, proposes cost effective investments for a sustainable programme of actions to deliver the targeted saving of lives whilst providing a framework to take advantage of any continuing central funding flows and initiatives. Local and national surveys show that public awareness of cancer symptoms is generally low not only for rarer cancers but also for common cancers except breast. In addition, although great improvements have been made in the last 10 years in establishing urgent referral pathways, only a minority of patients are referred through these pathways and delays continue to occur in the patient pathway. It is also important to ensure that improved access to specialist diagnostics once cancer is urgently suspected is maintained regardless of where the patient first presents, even though the majority of cancer diagnosis will be through the non-urgent referral route or as emergencies in A&E departments. The purpose of this strategy therefore is to impact on the behaviour of Londoners so that they present as early as possible to their doctor who should use evidence based treatment and care pathways to optimise and improve outcomes. 2. London Health Improvement Board – Cancer Prevention and Early Diagnosis Project The London Health Improvement Board (LHIB) has been established in shadow form, pending legislation, under the chairmanship of the Mayor, with the aim of improving the health of all Londoners. The Board has included the prevention and early diagnosis of cancer as one of its first priorities for action. This work stream will concentrate on tobacco control and smoking cessation for the prevention aspect of work and on enabling a London wide conversation about cancer to challenge existing attitudes of Londoners and aid earlier presentation. Close and careful integration of plans and project management will provide unique opportunities to save lives through the prevention and early diagnosis of cancer. 3. Aims and Objectives 3.1 Aim: To improve cancer survival through ensuring patients get diagnosed earlier. 3.2 Objectives: To increase public awareness of cancer symptoms To reduce perceived barriers to accessing primary care To enable/encourage earlier presentation To reduce inequalities To reduce the numbers of patients whose first presentation is in A&E To enable greater access for GPs to diagnostic tests and specialist advice to facilitate decision making and improve referral pathways To reduce the delays before diagnosis and treatment in secondary care To ensure that staging data are accurate and complete to enable effective monitoring To improve patient experience along the whole of the cancer pathway 3.3 Outcomes The expected outcomes are: Improved public awareness of cancer symptoms (as measured through CAM surveys or similar) Higher proportion of cancers referred through ‘2 Week Wait’ pathways Reduced emergency presentations with cancer. Higher proportion of people diagnosed with cancer at an earlier stage. Improved one and 5 year survival. However, these outcomes will not be known till some years later. Improved clinical pathways in primary and secondary care with reduced delays Improved access to and uptake of diagnostics from primary care A reduced economic and social impact from cancer on Londoners and London The aim is to save 1000 lives in London in line with the model of care. If survival across London matched the best in England, the table in appendix 1, summarised below, shows the number of lives that could be saved and illustrates the potential to meet the aim set by the model of care. Potential number of lives saveable Breast 325 Lung 576 Colorectal 388 Total 1289 However, it is recognised that improved prevention of cancer could save up to half of those lives currently lost and cancer prevention should remain an important priority 4. Baseline 4.1 Survival rates from cancer in London One year survival is recognised as being a reasonable proxy for late diagnosis. The latest available data are for people diagnosed in 2006-8 (cancer commissioning toolkit). One year survival from the main cancers, breast, colorectal and lung is widely variable across London with some of highest and the lowest rates in the country (Appendix 2). Five year survival is also highly variable. Two London PCTs (Barking & Dagenham and Waltham Forest) have both one and five year survival rates in the lowest national quintiles for all 3 cancers. Conversely 2 PCTs (Westminster and Hammersmith & Fulham) have one year survival rates in the highest national quintile for all 3 cancers. However, national rates are worse than international rates, so relatively good performance does not mean that improvement cannot be achieved. 4.2 Stage at presentation The aim of the NAEDI programme is to ensure that people present, are referred and diagnosed earlier. To measure whether this is happening, stage at diagnosis is an essential monitoring tool. Currently the availability of staging data is incomplete, with the extent of completeness varying from Trust to Trust and tumour to tumour. Although almost all solid tumours will be staged, clinically or pathologically, the data are not always recorded in a retrievable way and may not be routinely available. ICSs should be held to account for recording and routinely making available appropriate staging data. Thames Cancer Registry will have a key role in the collation of these staging data. 4.3 Co-morbidities and outcomes from cancer Good outcomes from cancer are also critically affected by the general health and comorbidities of patients. This emphasises the importance of overall prevention and health and wellbeing strategies such as those concerned with smoking, alcohol misuse, obesity and mental health (particularly in respect of depression and its impact on compliance with treatment). These factors may contribute to the poor outcomes regardless of stage at presentation. It will be essential to measure these co-morbidities if the impact of earlier detection initiatives is to be understood and intelligently targeted. 4.4 Population Awareness Population awareness of symptoms of cancer is vital to improving early diagnosis so that people know what to look for and when to go to their GP. Most cancer networks have conducted surveys of public awareness in their populations using the validated set of questions in the CRUK (Cancer Research UK) Cancer Awareness Measure (CAM) tool. NE London used the Breast CAM in 3 PCTs to focus specifically on breast cancer awareness, while NW London has used the Lung CAM in 2 PCTs. These surveys showed that only a small minority of people were able to spontaneously recall cancer symptoms other than lumps. Particular groups have been identified in local surveys as having lower levels of awareness – these include BME groups, lower socioeconomic groups, and males. People also perceived a range of barriers to accessing GPs if they thought they had a symptom. 4.5 Increasing Awareness of Cancer Symptoms All London cancer networks have initiated public awareness campaigns, using different methodologies, to raise public awareness. These have generally been targeted on specific tumour sites – bowel, breast or lung - and specific population groups. For example, 5 of the 6 London sectors have targeted bowel cancer, one has targeted breast and three lung cancer. In previous campaigns, three have targeted skin, one has targeted head and neck tumours and one has targeted oral cancer. The DH national campaign for bowel cancer awareness has been rolled out in early 2012 and local support was mobilised to maximise effectiveness. PCTs have bid for funding to pilot additional cancer awareness programmes centering on oesophogogastric, bladder and breast cancers in 2011-12. A further national campaign to raise awareness of lung cancer symptoms will be rolled out in May-June 2012. 4.6 Screening Cancer screening programmes make a significant contribution to early diagnosis. Uptake of all screening programmes is poorer in London than the national average with rates particularly low in Inner London PCTs. It is recognised that one important factor in low uptake is the high mobility of the population. However in 2009/10, no London PCT met the standard of 80% uptake for breast screening and only a third met the minimum standard of 70%. There have been substantial and encouraging increases in breast screening uptake in several London PCTs in the last year, particularly in East London where targeted campaigns have been initiated. For cervical screening only 3 PCTs met the minimum national standard of 80% coverage. 4.7 GP Referrals GP Audits Practice cancer profiles developed by NCIN provide a useful means by which practices can assess their referrals and cancer statistics against local and national benchmarks. GP audits of cancer cases in 2010 identified significant problems in the primary care stage of the pathway. Local audits supported national findings that a quarter of cancer cases present in A&E and around a fifth of cases have metastatic disease at diagnosis. Variation in GP Referral Patterns Nationally less than half (42%) of people with cancer were referred through the urgent two week wait (2ww) route (Cancer Waiting Times stats), whilst 23% came through A&E (National GP audit). In London there is large variation among PCTs in the proportion of cases coming via 2ww, from 22% (Hammersmith & Fulham) to 56% (Tower Hamlets) (Fig. 1). It is also true that there is variation within PCTs and between tumour sites and this needs to be analysed and understood if intelligence driven action is to be taken. In Newham, for example, the lower number of 2ww referrals for lung cancer is explained by the standard good practice pathway that fast tracks patients with suspicious chest X-rays direct to the specialist diagnostic pathway. Fig 1 GP referrals; % of cancer cases referred via 2ww, by PCT (source: Cancer Commissioning Toolkit) 60 50 40 30 20 TH Havering Redbridge WF B&D Camden Bexley Harrow Kingston CH Croyden Lambeth Greenwich Enfield Sutton and Merton Soutwark Barnet Islingtom Haringey R&Tw Lewisham Brent Bromley Newham Wandsworth Hillingdon Westminster K&C Ealing Houslow 0 Ham'th & Fulham 10 GP Training The level of GP training is usually a PCT led process and has been very variable between and within Networks. Most London networks are developing a comprehensive learning programme. Primary Care Leadership All Networks have a GP lead with varying time commitments and continuity of funding. £25,000 was made available in August 2011 by the DH for primary care leadership in all networks on a non-recurring basis for 2011/12. The number of GP leads is likely to change with the transition from PCTs into the emerging GP Clinical Commissioning Groups (CCG). Primary care leads are key to leading local actions with GPs. 5. Priorities for London Six priority areas have been identified for the earlier detection of cancer. Effectively implementing these priorities will need a whole systems mobilisation across London. It will need involvement and engagement of the public and communities, patient partnership groups, the business community, Local Authorities, Public Health services, the Third Sector in general and the Cancer Charities in particular, as well as the NHS including its primary, secondary and tertiary care and the Integrated Cancer Systems in particular. These priorities need to be explicitly commissioned and it will need the pan London agreement of commissioning intentions and the commitment of resources needed. Because of the socioeconomic and cultural diversity of London’s populations, priorities will need to be implemented with local design input to ensure success and to ensure that they do not, perversely, widen inequalities. Implementation plans will need to be clear on accountabilities and actions whilst ensuring that London’s ‘cancer stakeholders’ are involved. Implementation of these priorities will need to involve the sharing of best practice from England and from Europe as well as current findings from ongoing initiatives in London. This will be particularly important where local actions have focused on particular communities and population segments; evaluated actions can be spread across other parts of London where appropriate. All of the actions will need to consider best practice in service and process re-design and ‘Lean Thinking’. Information and Intelligence NAEDI (and all cancer commissioning) must be supported by high quality data and data analysis in order to: show evidence of need and target interventions show effectiveness of interventions support commissioning decisions that underpin NAEDI support Joint Strategic Needs Assessments (JSNAs) coordinate the analyses of ‘practice profiles’ and RCGP Audits monitor and report on output and outcome measures It would not be possible to develop or recommend appropriate interventions, or to assess them, without high quality data and data analysis support. In order to maximise quality and efficiency, this should be provided by a single, high quality team. This can be achieved by the collaboration of existing resources including, for example, intelligence and public health experts within the current cancer network teams, more general information analysts within London Health Programmes, performance management analysts for cancer in NHS London and, of critical importance, linking with the Thames Cancer Registry (TCR) and to the National Cancer Intelligence Network (NCIN). In particular it will be essential to have complete, accurate and timely staging data for all cancers to determine changes in presentation patterns together with the recording of emergency presentations of cancer through A&E. Commissioning of pathways and contracts with providers must reflect this requirement. A key deliverable, as a commissioning support tool, will be an ‘outcomes framework’ and reporting mechanism for earlier detection (in addition to the output specification metrics for the ICSs). This will need to align with national models, including NICE Quality Standards, and integrate with the output specification metrics for the Integrated Cancer Systems. This could include, for lung cancer as an example: 5 year survival 1 year survival curative resection rates stage at presentation emergency/A&E presentation rates lung cancer awareness measure scores % cancers referred through direct x-ray requests It will also be important to develop and agree metrics for measuring co-morbidities and to respond to the data collection arrangements for uptake of diagnostic tests from primary care as these are introduced by the Department of Health. Evidence-based Interventions to Improve Public Awareness Where there is good evidence for measures that support early diagnosis, these should be introduced across London. The evaluation of national and local pilots is contributing to the evidence base on effectiveness of public awareness campaigns. All areas will have local solutions for local issues but maximum health gain requires an overall pan London approach. These measures should include: Public awareness – The National Bowel Cancer Awareness Campaign ran for two months from the end of January 2012. A national lung cancer awareness will run for two months in May-June 2012. National campaigns require clear and careful panLondon and local implementation for maximum effect. DH/NCAT funded pilot projects with evaluation are underway for breast, bowel and lung cancer and more are in preparation for other tumour sites. DH is also funding pilot projects for campaigns to raise awareness of oesophagogastic cancers. These campaigns will require local ‘advocacy’ and engagement and possibly design modifications to ensure effective pan London spread and to ensure that they target groups identified as having poorer awareness. Presentation to primary care – Implementation of awareness campaigns needs to be mirrored with initiatives to ensure that people, in addition to being aware of the importance of their symptoms, present to primary care. These initiatives may be locally or population segment specific but remain an essential element of the pan London approach. Screening for breast, cervix and bowel cancer is critical to improving early detection and therefore to the commissioning strategy plans of commissioning groups. This is a particular area where the evaluation of local improvement strategies needs to be shared across London where communities and population segments can be shown to benefit from specific approaches. To maximise the effectiveness of these interventions, and the tackling of inequalities, we recommend a London wide approach. This may best be delivered by a small specialist team to ensure co-ordination and implementation and to support local action. GP Engagement and Service Improvement We recommend that each CCG has a primary care cancer lead (PCCL) with a minimum of one and up to 2 sessions per week for cancer work (to reflect population needs). The role of this post will include the need to improve early diagnosis and the most effective use of diagnostics through: raising awareness of and implementing London wide NAEDI initiatives locally identifying solutions to address local needs (in cancer) ensuring implementation and appropriate use of diagnostic pathways ensure maximum GP participation in education and training programmes: - Early diagnosis of cancer - Use of diagnostics GP involvement in the cancer pathway to include follow up where appropriate reviewing practice cancer profiles and carrying out local cancer audits. These may include audits such as: - Review of last 2 years cancer diagnoses looking for delays - Practice level audits of patient awareness - Root analysis of cancers diagnosed at A&E or by Acute Oncology Services (AOS) Macmillan Cancer Support have already made specific and updated recommendations on this within their role description of a Macmillan primary care cancer lead which has a wider remit beyond earlier detection. Direct GP Access to Diagnostics Direct access to the following should be available to and accessed by all GPs in London as per national guidance: chest X-Ray for lung cancer non obstetric ultrasound for pelvic gynaecological cancer, particularly ovarian cancer. MRI for brain tumours flexible-sigmoidoscopy and colonoscopy for colorectal cancer A survey of current commissioning arrangements has indicated that: all PCTs in London provide direct access to chest x-ray although access to x-ray through pathways that give rapid access to lung MDTs is variable all PCTs provide commissioned access to MRI and the large majority to non-obstetric ultrasound although uptake is variable and cancer specific usage is not known. direct access to flexi-sigmoidoscopy and colonoscopy is variable with local schemes and pilots This analysis of this baseline survey will be developed and validated through primary care leads and made available as a commissioning support tool. Most networks have highlighted the need for reviewing current access to diagnostics. In NE London and NC London, there are local projects to test direct access to colonoscopy. SW London is testing a direct pathway from pharmacy to secondary care for residents with suspect lung and bowel cancer symptoms; they are also testing direct access to sigmoidoscopy. Some localities are exploring models that give direct public access to diagnostic tests. As these investigations are primarily designed to diagnose cancer with the intent of improving outcomes, we have agreed the following principles: tests should be requested rapidly following presentation referral for the original test should be seen as the initiation of a diagnostic pathway, where abnormal findings should result in direct further investigations to diagnose or exclude cancer without unnecessary delays in the treatment pathway and with the minimum of hand offs to ensure all patients receive the highest quality care reports must be available in a timely manner (within one week). Requesting criteria for direct GP access to these tests and the pathways to general or specialist diagnostic services are being developed nationally and, when published by the DH, should be disseminated to all GPs. The DH recognise that data are not available on current GP use of such diagnostics for the specific indication of suspicion of cancer and are also developing data collection requirements which should be implemented across London once agreed. These diagnostic pathways will need to be commissioned to ensure access across London. This national strategy is intended to increase the use of these tests from primary care; PCTs should plan for this increase. The lack of an accurate baseline of current access and usage constrains the estimate of the cost impact. Role of Integrated Cancer Systems (ICS) in Reducing Delay Integrated cancer systems are being developed across London and are an integral part of achieving earlier detection from cancer. Earlier diagnosis and better survival at 1 year should be key performance indicators for the ICS. The ICS will need to work with CCGs, Networks and others across the whole of the early detection pathway but with a particular emphasis and leadership role on optimising referral from primary care. ICS will need to ensure all trusts with specialist cancer services have acute oncology services to ensure patients presenting with symptoms suspicious of cancer are investigated on an enhanced pathway. Presentation with cancer as an emergency will be seen as a key indicator of improving earlier detection of cancer. All trusts should have clear protocols for scrutiny and transfer of patients with symptoms suggestive of cancer to an enhanced pathway. ICS should be commissioned to record and report stage at presentation and the number of presentations of cancer as emergencies. Output metrics should also include measures of co-morbidities. 6. Resources The cost of cancer in England, including both direct NHS costs and societal costs such as the loss of productivity, has been estimated at approximately £18 billion per annum (Featherstone and Whitham, Policy Exchange 2010). The same source proposes that if UK survival rates improve to the best in Europe then a substantial reduction in cost will result, £10 billion cumulatively by 2020. These economic benefits will be available to, and important for, London and Londoners. The DH financial impact assessment of the NAEDI strategy, published in January 2011, sets out detailed cost modelling and analysis of the impact of earlier diagnosis on five different cancers. There is likely to be increases in diagnostic costs partially offset by a smaller reduction in treatment costs. They also recognise the additional increase in diagnostic and treatment costs while the new policy is implemented. This is the time when the period between the onset of the disease and the diagnosis is reduced and there is a catch up to meet the new times. Their overall conclusion is that earlier detection would represent value for money but would not be cost saving. This is consistent with the conclusion reached in the model of care. There are difficulties and variability in estimating these effects; this variation has been illustrated in the evaluation of the pilot of the national bowel awareness campaign when the increase in screening uptake has not reached the anticipated levels. The DH work is based on national statistics, the impact on London needs to be better understood given for example the lower levels of screening uptake that have been resistant to repeated efforts to improve them. The financial impact will also depend on the speed at which implementation, including for screening, is planned and delivered. The next stage of analysis will be to take the model used by the DH and use data and assumptions that are appropriate for the capital so that the overall financial impact can be included in a business case. It is recommended that commissioners should: Allow for an expected increase in use of diagnostic and treatment costs in risk reserves for 2012-13 until detailed plans are developed Include provision in commissioning strategy plans for awareness campaigning at the level of £100,000 per 200,000 population, network GP leadership at £25,000 per network and up to 2 sessions per CCG 7. Commissioning Support Tools The following are being developed to provide more detailed information to support commissioning of earlier detection: a) Summary of delivery responsibilities for key elements of strategy b) Summary of recommendations and commissioning intentions c) Early detection pathways with evidence base and best practice interventions. The programme will explore the development of these on Map of Medicine. The initial priority will be for colorectal (extract of project initiation document appended no its not), lung cancer, ovarian cancer and brain cancer reflecting the priority open access diagnostic tests. These will provide templates for a development programme for other cancers. d) Validated analysis, by PCT, of availability and commissioning of direct access to the four priority diagnostic tests e) Requesting/referral criteria and pathways for the priority diagnostic tests as they are issued by the Department of Health f) Department of Health economic models localised for London g) A framework of monitoring metrics and reporting process 8. Implementation plan An outline implementation plan and delivery model is shown below. This will require further development. It is important to acknowledge that the delivery model for earlier detection is complex and this is particularly the case as the NHS transitions to the new commissioning arrangements and, for London, the integrated cancer systems develop. Implementation plans will require further development as changes emerge and to ensure clarity on leadership and responsibility and accountability for actions. It is proposed that the current lead arrangements for the London cancer programme continue during the transition and for the overall coordination of the implementation of this strategy reporting to the proposed London (Commissioning) Cancer Board as it emerges. Current lead arrangements within cancer networks and at borough and cluster levels, reporting to network boards, should continue in the transition with clear links to the London level programme. Or: It will be important to maintain the local leadership at borough and cluster level through and beyond the transition; these will need to have clear links with the London Programme. Successfully achieving the lives saved targeted by this strategy will require the integrated actions of existing and emerging NHS structures including Health and Well Being Boards, The NHS Commissioning Board and Clusters, Cancer Networks, Integrated Cancer Systems, Public Health England, the London Screening Improvement Board, Clinical Commissioning Groups and Primary Care. It will particularly need the careful integration with other strategies including those of the LHIB and the London Screening Improvement Board. Priority Lead Timescale PT Apr 2012 Accurate and complete recording of staging and A&E presentations to be included in all commissioning contracts SCUs Mar 2012 Pathways and best practice guides PT Dec 2011 to Sept 2012 All areas of London to have plans to raise public awareness of cancer, with a London wide project team to co-ordinate Networks/PT Sept 2012 Ensure all social marketing campaigns are properly evaluated and that evaluations are used to provide an evidence base for effectiveness Networks 1. Information and Intelligence Develop outcomes framework of metrics and reporting process 2. Improving awareness of cancer Ongoing 3. GP Engagement and Service Improvement All areas to have GP cancer leads CCGs Apr 2012 All areas to have rolling programme of integrated training programmes for GPs to keep GPs up to date with guidance CCGs ? Apr 2012 GPs to be encouraged to audit pathways of all cancer cases GP leads Ongoing AOSs* to audit all people with cancer first presenting at A&E to identify reasons ICSs Ongoing from Dec 2011 SCUs/CCGs Apr 2011 PT Oct 2012 ICSs Dec 2011 ICSs Apr 2012 ICSs Ongoing 4. Improving GP access to diagnostics Commission direct access for GPs to specified diagnostics with direct onward referral for positive cases; CXR Flexible sigmoidoscopy/colonoscopy Non Obstetric US for ovarian cancer MRI for suspected brain cancers Disseminate protocols/guidance for direct access and for results pathways 5. Reducing delays in secondary care All A&E departments and trusts with specialist cancer services to have an acute oncology service to pick up patients with suspected cancer as per national guidelines All acute trusts to have protocols and training for the rapid pathway to ensure all patients with suspected cancer are transferred to the appropriate clinical dept irrespective of their route into the trust including A&E and routine medical and surgical All trusts should regularly audit their cancer pathways by tumour site against international best practice and to identify system delays Commissioners to monitor compliance with contract SCU/Networks Ongoing LHIB Ongoing PT Jun 2012 LHIB Focusing on the interventions proposed within prevention and early diagnosis workstream www.lhib.org.uk Resources Localise DH economic models to London and analyse results *SCU = Sector Commissioning Unit AOS = Acute Oncology Service ICS = Integrated Cancer system PT = Early Detection project team Appendix 1. Potential numbers of lives saved in London These have been calculated by taking the best 5 year survival rates for breast colorectal and lung in the country and applying them to cancer populations in London PCTs. These calculations suggest that over 1200 lives could be saved in London for these 3 cancer sites. Given the complexities of European comparisons, choosing the best in England as a target seems a more robust benchmark in the short term but aiming for survival rates that compare to the best in Europe should remain the target. These figures are only indicative and should not be taken as target figures. Additionally there is considerable variation within boroughs, eg borough with good survival may have pockets of poor survival Breast Colorectal Sum of breast, colorectal and lung Lung Lives Lives Lives Incidence saved Incidence saved Incidence saved 2002-4 pa 2002-4 pa 2002-4 pa cases pa Lives saved pa Barking and Dagenham 286 14 239 21 339 16 288 52 Barnet 586 10 437 36 425 13 483 59 Bexley 485 11 356 21 406 14 416 46 Brent 387 6 317 16 318 10 341 32 Bromley 728 11 491 37 526 22 582 70 Camden 311 4 248 14 292 6 284 25 City &Hackney 263 15 199 5 284 9 249 29 Croydon 654 13 433 20 451 20 513 53 Ealing 452 13 342 20 359 13 384 46 Enfield 475 15 377 31 364 16 405 61 Greenwich 389 9 368 30 418 18 392 58 Hammersmith and Fulham 214 6 162 11 234 10 203 28 Haringey 297 10 223 8 264 9 261 27 Harrow 443 9 274 14 256 7 324 30 Havering 501 14 409 27 451 20 454 61 Hillingdon 408 10 260 17 402 17 357 43 Hounslow 314 13 262 17 265 10 280 40 Islington 229 8 212 14 318 12 253 34 Kensington and Chelsea 271 3 204 4 197 0 224 7 Kingston upon Thames 307 2 240 15 192 8 246 25 Lambeth 409 11 277 15 361 13 349 40 Lewisham 396 12 277 24 375 14 349 50 Newham 269 15 193 13 322 13 261 41 Redbridge 417 13 321 20 315 10 351 43 Richmond upon Thames 378 7 285 14 278 10 314 31 Southwark 383 13 275 23 394 18 351 54 Sutton & Merton 663 17 566 30 548 19 592 66 Tower Hamlets 224 11 190 9 337 10 250 30 Waltham Forest 309 15 249 28 265 14 274 57 Wandsworth 442 9 303 23 385 13 377 45 Westminster, 358 7 238 0 318 1 305 9 388 10711 1289 London 325 576 * Using numbers of people diagnosed in 2002-4 and 5 yr survival rates for people diagnosed in 2002-4; NCIN G L LO AN N D Ke D n s H ON 'n ar & ro C w he ls e Ba a rn Br et om le B y R ren ic h t R mon ed br d id g Ea e l in W M g e s er tm ton in s C te r ro , yd o En n H f iel il li d n H gdo ar n in Ki ge y ng st W on al S t H ham ut to am n 'th Fo & res Fu t H lha av m H eri n ou ns g lo Be w x C le y am H de n ac Le kn w ey is h N am W ew a n ha ds m G wo re rth e So nwi u t ch hw La ark m be Ba rk Is l th in in g g To & to n w er Dag H am 'm le ts EN Age standardised registration rate per 100,000 G LA Ke n s LO ND 'n N & DO C he N ls e W Ha a e s rro tm w in st er , So Bre u t nt hw ar Ba k rn Ba rk Be et in g xle & y D R ag ed 'm br id ge To w En er f ie H ld a G ml re e t en s w i Br ch om N le ew y ha C m am H de il li n ng H do av n e W Lew ri ng al th i sh am am Fo re s Ea t La l ing m b H et ar h in ge W Su y an tt ds on w or H am Ha th 'th ckn & ey Fu lh a M m er C ton ro yd Ki o n ng H sto ou n ns lo Is w lin R gto ic hm n on d EN Age standardised registration rate per 100,000 G LA LO N D N D O N Br e H nt ar ro w En f ie To ld w Ba er rn H et am So le ut ts hw ar Be k xl N ey ew h H am a G ckn re e en y w Ke ic ns h 'n E & al i C ng he ls e Su a H t ton W ari e n W stm ge y al th i ns am te r Fo , re M st e H Ho rto am u n 'th ns & low Fu lh La a m m b H et il li h ng d C on am C de n ro yd Ba o rk Bro n in g ml e & y D Le ag w 'm is R ham ed br i H d ge av er Is i ng lin R gto i W chm n an o ds nd w o Ki rth ng st on EN Age standardised registration rate per 100,000 Appendix 2. Cancer incidence rates in London boroughs Appendix 2 shows the incidence rates for breast colorectal and lung cancer in London boroughs. These rates are age standardised so variations in numbers of cases due to an older or younger population are evened out. Incidence rates demonstrate health inequalities between boroughs in London 160 Incidence of breast cancer in London boroughs, 2006-8 140 120 100 80 60 40 20 0 70 Incidence of colorectal cancer in London boroughs, 2006-8 60 50 40 30 20 10 0 Incidence of lung cancer in London boroughs, 2006-8 90 80 70 60 50 40 30 20 10 0 Appendix 3. One and 5 year relative survival rates from breast, colorectal and lung cancers, national quintiles, in London PCTs One year survival* Organisation name Breast Colorectal Lung 5 year survival* Breast Colorectal Lung Barking and Dagenham PCT 93.37 69.7 24.13 76.53 43.12 6.08 Barnet 96.75 74.12 31.62 86.49 45.1 11.33 Bexley Care Trust 98.56 72.03 25.58 84.92 52.62 9.64 Brent Teaching PCT 94.51 78.39 32.7 86.99 54.91 11.01 Bromley PCT 96.43 73.25 34.6 87.12 47.61 7.58 Camden PCT 94.66 82.69 32.99 87.4 53.39 13.69 City and Hackney PCT 96.59 69.82 29.2 74.37 62.53 10.75 Croydon PCT 95.71 78.28 34.97 85.73 56.38 6.94 Ealing PCT 95.58 74.4 26.98 82.92 52.65 9.14 Enfield PCT 94.59 73.23 30.89 82.24 45.37 7.34 Greenwich Teaching PCT 94.44 73.3 28.24 84.36 45.48 7.23 Hammersmith and Fulham 98.95 78.29 35.83 83.15 49.49 6.87 Haringey Teaching PCT 96.78 70.67 35.27 81.99 58.67 10.18 Harrow PCT 95.21 69.75 33.11 85.73 55.1 11.73 Havering PCT 96.08 68.44 32.27 83.33 50.42 6.95 Hillingdon PCT 95.53 74.32 21.67 84.51 50.3 7.86 Hounslow PCT 99.27 76.96 30.15 79.22 50.1 9.02 Islington PCT 93.44 72.59 35.1 81.39 49.87 8.7 Kensington and Chelsea PCT 96.02 81.82 43.49 88.44 63.74 20.31 Kingston PCT 97.88 80.87 33.98 89.5 51.6 7.07 Lambeth PCT 97.83 72.37 33.85 83.31 53.36 9.48 Lewisham PCT 97.04 68.76 30.73 82.69 44.24 8.84 Newham PCT 95.3 65.88 28.45 75.05 49.34 8.05 Redbridge PCT 96.09 74.35 26.4 82.6 50.9 10.72 Richmond and Twickenham 96 80.89 38.22 86.19 55.45 9.32 Southwark PCT 95.62 80.25 33.25 81.42 45.11 6.81 Sutton and Merton PCT 96.09 71.82 37.45 84.03 54.21 9.65 Tower Hamlets PCT 92.99 70.85 32.17 76.42 56.31 11.56 Waltham Forest PCT 93.57 68.97 27.04 77.03 36.73 4.38 Wandsworth PCT 97.9 76.78 31.89 85.22 47.16 10.45 Westminster PCT 97.37 80.55 42.96 85.64 70.04 18.9 * People diagnosed in 2006-8 (one year), and 2002-4 (5 year). Source: CCT Lowest quintile Highest quintile