Sample Monthly Inspection
advertisement

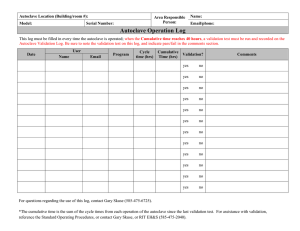
Treatment and Disposal of Biohazardous Waste UBC.RMS.ENV.001.PRO Date of Issue: Procedure Autoclave Facilities Sample Monthly Inspection Checklist 13.09.26 Building name: Room #: Autoclave Make & Model: Unit Serial #: Inspection date Inspector’s contact information: Name Phone E-mail Instructions: 1. 2. 3. 4. 5. Complete inspection on a monthly basis. Inspect each item on the checklist and check Yes box ( ) if satisfactory or No if unsatisfactory. For unsatisfactory items, describe the deficiency in the Comments section. Take actions or make necessary recommendations to correct the deficiencies. Submit a copy of the completed checklist to RMS at the end of each month, through the autoclave.report@ubc.ca email Checklist Items Yes No 1. Does the room have a controlled Access? ☐ ☐ 2. Room is open but area/floor is controlled ☐ ☐ 3. Is the area inspected monthly? ☐ ☐ 4. Record of inspection is up-to-date? ☐ ☐ 5. The area is free of spills and leaks? ☐ ☐ 6. Autoclave cycles are recorded on autoclave logs? ☐ ☐ 7. Autoclave Charts are kept on file? ☐ ☐ 8. Written autoclave logs contain all required information? ☐ ☐ 9. Has the autoclave unit been tested with biological indicator (BI) monthly? ☐ ☐ Date BI was tested (mm-dd-yyyy) Comments If YES please provide date and serial # below. Vial lot (serial) # 10. Was the test successful this month? ☐ ☐ 11. Were the BI test parameters (temperature=121°C, time=60min, pressure=15psi) noted on the autoclave log? ☐ ☐ Inspector’s signature: ______________________________