RESEARCH PROTOCOL
advertisement

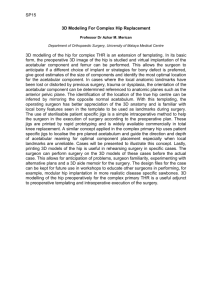
ARTHRITIS AND JOINT REPLACEMENT CENTER PHILIPPINE ORTHOPEDIC INSTITUTE Makati City RESEARCH ARTICLE TITLE : CRITICAL ANALYSIS OF SIXTY FIVE (65) HIP REVISION CASES IN A PERIOD OF TWENTY THREE YEARS (1987-2008) AUTHOR : Marcelino T. Cadag, MD ; Ramon B. Gustilo, MD ; Liberato Antonio C. Leagogo, MD ABSTRACT Background: Over a thousand Joint Replacement Surgeries have been done by surgeons (Gustilo/Leagogo) of the Philippine Orthopedic Institute in the Philippines since its inception over 20 years ago. Revision surgery of failed cemented hip replacement, have been increasing in the last decade and constitute 7% of all joint replacement surgeries performed. Materials and Methods: All medical records of the patients were reviewed to determine the following: 1. Etiology 2. Duration from index surgery 3. Common anatomical pathology and amount of leg length discrepancy encountered. 4. Revision implants used and use of allograft. 5. Postoperative course and complications 6. Preliminary results (How many are ambulatory with or without assistive device). 7. Analysis of x-ray at last follow-up (two years minimum). Results: A total of sixty five (65) patients were included in the study. Forty four (44/65) patients (67.7%) underwent revision due to aseptic loosening of components and osteolysis (femoral or acetabular). Ten (10/65) patients (15.4%) developed infection. Three (3/65) patients (4.6%) developed protrusio acetabuli that necessitated revision. Periprosthetic fracture was noted in three (3/65) patients. Another three (3/65) had implant failure. Two (2/65) patients (3%) had hip dislocation prior to revision. Average number of years from index surgery is 6.44 years (1-19 years) for loosening and osteolysis, and 9 years (1-20 years) for infection. Fifty seven (57) patients (87.7%) underwent cemented total hip prior to revision while eight (8) patients (13.3%) underwent cemented partial hip replacement prior to revision. Fifty six (56) patients (81%) have shortening on the affected side with an average of 3cm (1-6cm). Twenty five (25) patients (38.5%) had proximal femoral bone loss requiring structural allograft. Twenty one (21) patients (32.3%) had acetabular defect (Paprosky Types I & II) but only nine (9) required compaction bone grafting. In forty five (45/65) patients (69.2%), cementless (ReflectionTM) cup was used. Cementless, modular, revision stem (Active LockTM) was used in twenty nine (29/65) patients (44.6%). All patients were allowed full weight-bearing after revision surgery. Four patients (6%) developed acute post-op infection. Two patients (3%) had dislocation after revision surgery. Functional results at short-term follow-up (two years minimum [4.4 years average]), were excellent (ambulatory without assistance) in 52.4%, good (ambulatory with assistive device) in 43%, and poor (non-ambulatory) in 4.6%. Follow-up radiographs showed implants in excellent alignment, no signs of loosening, migration or subsidence. Conclusions: The main reason for revision hip arthroplasty is aseptic loosening (67.7%) followed by infection (15.4%). The use of long non-cemented, modular, calcar-replacing curved revision stem, and strut allograft on the femoral side; jumbo, cementless cup with compaction bone grafting on the acetabular side, addressed the problem of anatomic pathologies as a result of failed, cemented THR. Good to excellent functional results in 95.4% at short-term (>2 years) follow-up. There is no association between cause for revision with gender and age of the patients. Long term follow-up study is still ongoing. INTRODUCTION: The need for revision arthroplasty is steadily rising. In the United States, the rate of revision total hip arthroplasty increased by 3.7 procedures per 100,000 persons per decade, and that of revision total knee arthroplasties, by 5.4 procedures per 100,000 persons per decade1. In a related study in the US, The demand for hip revision procedures is projected to double by the year 2026, while the demand for knee revisions is expected to double by 2015. Overall, total hip and total knee revisions are projected to grow by 137% and 601%, respectively, between 2005 and 20302. The mean total hospital cost for revision hip surgery in the United States, back in 2005, is $31,3413. The most recent epidemiological study on revision hip surgery in the United States found out that the average hospital stay was 6.2 days and the average total charges was $54,533 4. Hospital charges for revision total hip arthroplasty and revision total knee arthroplasty were projected to increase by 290% to $3.8 billion and by 450% to $4.1 billion5. However, there are no available data on the prevalence of revision arthroplasty in the Philippines. This study aims to describe cases of hip arthroplasty that necessitated revision surgery, in terms of problems presented, etiology, duration from index surgery, anatomical pathology, surgical approach, choice of implant, antibiotics used, post-operative course and complications, preliminary results and analysis of radiographs at last follow-up. We will also determine if there’s an association between cause for revision hip surgery with gender and age of the patients. MATERIALS AND METHODS: We reviewed the medical records of adult patients seen at the Philippine Orthopedic Institute (POI) who underwent hip joint reconstruction in affiliated hospitals, developed early or late complications and underwent revision surgery for the past twenty (20) years. A total of sixty five (65) patients were included in the study. Patient Demographics There were 76 patients initially but only 65 had minimum of 2 years followup. There were 44 females and 21 males. Average age is 58.4 years (18-85 years). Etiology Forty four (44/65) patients (67.7%) underwent revision due to aseptic loosening of components and osteolysis (femoral or acetabular). Ten (10/65) patients (15.4%) developed infection. Three (3/65) patients (4.6%) developed protrusio acetabuli that necessitated revision. Periprosthetic fracture was noted in three (3/65) patients. Another three (3/65) had implant failure. Two (2/65) patients (3%) had hip dislocation prior to revision. (Table 1) Table 1. Etiology for Revision Hip Surgery CAUSE OF REVISION NUMBER OF CASES PERCENTAGE Aseptic Loosening Infection Protrusio Acetabuli Periprosthetic Fracture Implant Failure Dislocation 44/65 10/65 3/65 3/65 3/65 3/65 67.7% 15.4% 4.6% 4.6% 4.6% 3% Duration from index surgery The average number of years from index surgery is 6.44 years (1-20 years). For loosening and osteolysis, the average is 4.6 years (1-19 years), and 9 years (1-20 years) for infection. Anatomical Pathology Fifty six (56) patients (81%) have shortening on the affected side with an average of 3cm (1-6cm). Twenty five (25) patients (38.5%) had proximal femoral bone loss requiring structural allograft. Twenty one (21) patients (32.3%) had acetabular defect (Paprosky Types I [57%] & Type II [43%] ) but only nine (9) required compaction bone grafting. Revision Implants Used In forty five (45/65) patients (69.2%), cementless (Reflection TM) cup was used. Cementless, modular, calcar-replacing, curved revision stem (Active LockTM) was used in twenty nine (29/65) patients (44.6%). Cemented stem was used in 24 patients (37%), and cemented cup in 11 patients (17 %). We retained the cup in 8 patients (12.3%), and retained the stem in 11 patients (17 %). RESULTS: Since 1984, the most number of hip revision surgery performed was in 1997 with nine (9) cases, the number of cases dropped in 1998 with only one revision surgery. From then, there was a gradual increase in number of cases until 2005 and a decreasing trend until 2007 (Figure 1). The age group with most number of revision cases was the 40 - 79 year old group, and the least were the group of patients less than 40 years and more than 80 years (Figure 2). Number of Patients with Hip Revision Surgery Per Year 10 9 Number of Patients 8 7 6 5 4 3 2 1 2002 2003 2004 2005 2006 2007 2002 2003 2004 2005 2006 2007 2001 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 1987 1986 1985 1984 0 Year of Revision Number of Patients Figure 1. Distribution of Patients Per Age Group Per Year Number of Patient 5 4 3 2 1 2001 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 1987 1986 1985 1984 0 Year of Revision 1 - below 30 2 - 30 - 39 3 - 40 - 49 5 - 60 - 69 6 - 70 - 79 7 - 80 and above 4 - 50 - 59 Figure 2. More hip revision surgery were performed in women than men (200%), and this has been constant since 1991 – 2007 (Figure 3). As previously stated, the main cause of hip revision surgery was aseptic loosening followed by infection. (Figure 4). Gender Distribution Per Year of Patients Who Underwent Hip Revision Surgery 6 Number of Patient 5 4 3 2 1 2001 2002 2003 2004 2005 2006 2007 2001 2002 2003 2004 2005 2006 2007 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 1987 1986 1985 1984 0 Year of Revision 1 - Male 2 - Female Figure 3. Causes of Hip Revision Surgery Per Year 10 8 7 6 5 4 3 2 1 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989 1988 1987 1986 1985 0 1984 Cause of Revision 9 Year of Revision 1 - aseptic loosening 2 - protrusio acetabuli 3 - infected THA 4 - others (hip dislocation, periprosthetic fracture) Figure 4. Statistical Analysis Chi-square test for independence (Pearson chi-square) with 5% level of significance, was used to determine if there’s an association between the cause of revision, with the gender of the patients. A. Association Between Reason for Hip Revision Surgery and Gender Crosstab Hip Revision Surgery As eptic Loosening Protrus io Acetabuli Infected THA Others Total Count % within Hip Revision Surgery Count % within Hip Revision Surgery Count % within Hip Revision Surgery Count % within Hip Revision Surgery Count % within Hip Revision Surgery Gender Male Female 15 29 34.1% 65.9% Total 44 100.0% 3 3 100.0% 100.0% 4 4 8 50.0% 50.0% 100.0% 2 8 10 20.0% 80.0% 100.0% 21 44 65 32.3% 67.7% 100.0% Crosstab Hip Revision Surgery As eptic Loosening Others Total Count % within Hip Revision Surgery Count % within Hip Revision Surgery Count % within Hip Revision Surgery Gender Male Female 15 29 Total 44 34.1% 65.9% 100.0% 6 15 21 28.6% 71.4% 100.0% 21 44 65 32.3% 67.7% 100.0% Chi-Square Tests Pearson Chi-Square Continuity Correction a Likelihood Ratio Fis her's Exact Test Linear-by-Linear As sociation N of Valid Cases Value .198b .026 .200 .195 df 1 1 1 1 As ymp. Sig. (2-sided) .656 .872 .654 Exact Sig. (2-sided) Exact Sig. (1-sided) .780 .441 .659 65 a. Computed only for a 2x2 table b. 0 cells (.0%) have expected count less than 5. The minimum expected count is 6.78. We can see that at 95% level of significance, a p-value of 0.780 is not significant (greater than 0.05). This means there is no association between gender and revision hip surgery. The Fisher’s Exact Test with 5% level of significance, was used to determine if there’s an association between cause of revision and age of the patients. B. Association Between Reason for Hip Revision Surgery and Age Descriptive Statistics Hip Revision Surgery (Age) Aseptic Loos ening Protrusio Acetabuli Infected THA Others N 44 3 8 10 Minimum 18 55 36 43 Maximum 87 78 80 85 Mean 56.23 67.67 57.63 65.80 Std. Deviation 14.48 11.68 18.02 11.97 Age * Hip Revision Surgery Crosstabulation Age 60 and below above 60 Total Count % within Age Count % within Age Count % within Age Hip Revision Surgery As eptic Loosening Others 29 8 78.4% 21.6% 15 13 53.6% 46.4% 44 21 67.7% 32.3% Total 37 100.0% 28 100.0% 65 100.0% Chi-Square Tests Pearson Chi-Square Continuity Correction a Likelihood Ratio Fis her's Exact Test Linear-by-Linear As sociation N of Valid Cases Value 4.485b 3.422 4.485 4.416 df 1 1 1 1 As ymp. Sig. (2-sided) .034 .064 .034 Exact Sig. (2-sided) Exact Sig. (1-sided) .060 .032 .036 65 a. Computed only for a 2x2 table b. 0 cells (.0%) have expected count less than 5. The minimum expected count is 9.05. At 95% level of significance, there is no association between hip revision surgery and age (p-value=0.06 is greater than 0.05). Post-operative and Clinical Outcome All patients were allowed weight-bearing as tolerated with walker or cane, after revision surgery. Four patients (6%) developed acute post-op infection. Two patients (3%) had dislocation after revision surgery. Functional results at short-term follow-up (two years minimum [4.4 years average]), were excellent (ambulatory without assistance) in 52.4%, good (ambulatory with assistive device) in 43%, and poor (non-ambulatory) in 4.6%. Sixteen (16) patients (24.6%) had more than 1 revision surgery and one (1) patient developed a chronic draining sinus who later underwent resection arthroplasty. Analysis of Radiographs at Last Follow-up Follow-up radiographs showed implants in good alignment, no signs of loosening, migration or subsidence. There were six (6) patients (9.2%) who developed heterotopic ossification (HO) around the hip joint but did not affect the functional outcome of the patients. DISCUSSION: Aseptic loosening secondary to wear-debris-induced osteolysis has been identified before, as the leading cause of late failure of total hip arthroplasty6. Osteolysis can be divided into several categories: patient-specific, implantspecific, and the result of surgical factors7. With recent advances in polyethylene manufacturing and processing, alternative bearing surfaces, implant design, early clinical results are encouraging, demonstrating 50% to 81% decreases in radiographic wear rates8. It is well known that wear particles are the primary driving force in aseptic loosening of orthopedic implants. Wear particles are generated by the primary articulation between the polyethylene liner and the metal head, as well as from the metal back and polyethylene insert. Considerable evidence has emerged demonstrating that various other factors can modulate the biologic activity of orthopedic wear particles. Two of the most studied modulating factors are bacterial endotoxins and implant motion9. Infection is fairly common in primary arthroplasty cases, and has a higher incidence in revision surgery. In the management of infected implant sites, antibiotic-impregnated cement used in one-stage exchange arthroplasties has lowered reinfection rates. In two-stage procedures, use of beads and either articulating or nonarticulating antibiotic-impregnated cement spacers also has lowered reinfection rates. Spacers also reduce "dead space," help stabilize the limb, and facilitate reimplantation. Problems associated with antibioticimpregnated cement in total joint arthroplasty include weakening of the cement and the generation of antibiotic-resistant bacteria in infected implant sites10. Implant design and positioning are important factors in maintaining stability and minimizing dislocation after total hip arthroplasty. Recent prosthesis designs can cause intra-articular prosthetic impingement within the arc of motion required for normal daily activities and thus lead to limited motion, increased wear, osteolysis, and subluxation or dislocation. Minimizing impingement involves avoiding skirted heads, appropriate size of the head and acetabular implant, maximizing the head-to-neck ratio, and, when possible, using a chamfered acetabular liner and a trapezoidal, rather than circular, neck cross-section. Computer modeling studies indicate the optimal cup position is 45° to 55° abduction. Angles <55° require anteversion of 10° to 20° of both the stem and cup to minimize the risk of impingement and dislocation11. Recently, in the United States, the most common causes of hip revision were instability/dislocation (22.5%), mechanical loosening (19.7%), and infection (14.8%)4. And the most common type of revision total hip arthroplasty procedure performed was all-component revision (41.1%)4. Revision surgery of failed cemented total hip can be approached systematically. On the femoral side, the problem of aseptic loosening and bone loss may be solved by using a fully-coated, curved, modular revision system and strut allograft augmentation. Modular femoral component systems typically provide accurate bone preparation through independent proximal metaphyseal machining (milling) and distal reaming providing improved line-to-line preparation. This facilitates precise fit and fill that allows for reliable and accurate seating of the femoral component, enhancing more accurate reproduction of appropriate neck offset, length, and version. In addition, the ActiveLockTM technology provides a unique locking strength that does not generate metallic wear debris (fretting). This technology also allows the component position to be adjusted intraoperatively which can be advantageous when doing revision surgery. On the acetabular side, the problem of aseptic loosening and bone loss remains to be a challenge. In this study, two treatment options were used, a jumbo cementless acetabular socket and a regular cementless acetabular cup placed superiorly, relative to the true hip center (high hip center). In the presence of severe acetabular bone loss, other treatment options include the use of an anti-protrusio cage, an oblong cup and structural allograft. In one report, a custom triflange acetabular prosthesis was used to treat massive acetabular bone loss and pelvic discontinuity in twenty eight (28) consecutive patients (30 hips), and provided a durable solution with good clinical results12. Ideally, the true hip center should be restored to address both the shortening and the biomechanical imbalance brought about by an eccentric (high) hip center. In this study, the problem of shortening and leg length inequality was addressed by using a calcar-replacing stem, a +10 femoral head, a thick, eccentric, off-set acetabular liner and by restoration of the true hip center. Revision hip arthroplasty entails a lot of surgical skills and financial burden to patients. In one study done in the US, hospital resource utilization for revision total hip arthroplasty was found to be significantly higher than that for primary arthroplasty3. The economic and clinical impact of revision total hip surgery in the Philippines is beginning to dawn.The cost of revision total hip surgery, let alone primary total hip surgery, is too much for the average Filipino (GDP per capita of $3,200). Clinically, only a handful of surgeons are equipped with the proper training, knowledge, experience and skills to perform revision hip surgery in the Philippines. Proper indication for primary total hip surgery, proper surgical technique (including asepsis and antisepsis), appropriate implant selection, good cementing technique and adequate surgical prophylaxis, all contribute to reduction of cases requiring revision hip surgery. Considering the economic and clinical burden of revision total hip surgery, doing a good primary total hip surgery is paramount in preventing future revisions. All total hip systems are designed to last for 10-15 years, but we found out in this study that average number of years from index surgery to revision is much less (6.4 years) than expected. Factors that may affect long term outcome of arthroplasty include surgical approach, technical expertise of surgeon, duration of operation, choice of implant, cementing technique, condition of bone stock, administration of antibiotics and pre-existing medical condition of the patient. Cementless acetabular system has been used extensively in primary total hip as well as revision surgery. However, the problem of polyethylene wear brought about by metal-backing (backside wear) has yet to be addressed. Backside wear can be significantly reduced by improving the locking mechanism of the polyethylene insert to the metal back acetabular socket. Presently, all cementless acetabular systems use the “press-fit”, passive locking mechanism. The development of a better locking mechanism remains to be an engineering challenge. Alternative bearing surfaces, such as highly cross-linked polyethylene, ceramic-on-ceramic, and metal-on-metal articular surfaces, have been introduced in an attempt to reduce wear and osteolysis following total hip arthroplasty. Intermediate-term follow-up data available suggest that the prevalence and severity of osteolysis may be reduced with these materials compared with conventional metal-on-polyethylene bearing surface couples. However, long-term data are presently unavailable; the future performance of these bearings awaits clinical validation13. Currently, only alumina-on-alumina bearings can claim virtually no biologic risk14. CONCLUSIONS: The main reason for revision hip arthroplasty in the Philippines is aseptic loosening (67.7%) followed by infection (15.4%), protrusio (4.6%), periprosthetic fracture (4.6%), implant failure (4.6%) and dislocation (4%). The use of long, modular, noncemented, calcar-replacing, curved revision stem, with the use of strut allograft, addressed the problem of anatomic pathologies on the femoral side as a result of failed, cemented THA. On the acetabular side, jumbo, cementless cup with compaction bone grafting, and eccentric placement of the hip center, addressed the problem of loosening and bone loss. The use of an Anti-Protrusio Cage (APC), oblong cup, and structural allograft, in revision of the acetabular side is very promising. Good to excellent functional results in 95.4% at short-term (>2 years) follow-up. There is no association between cause for revision with gender and age of the patients. Doing a good primary total hip surgery is paramount in preventing future revisions. BIBLIOGRAPHY: 1. Prevalence of Primary and Revision Total Hip and Knee Arthroplasty in the United States From 1990 Through 2002 J. Bone Joint Surg. Am., Jul 2005; 87: 1487 - 1497. 2. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030 J. Bone Joint Surg. Am., Apr 2007; 89: 780 - 785. 3. Hospital Resource Utilization for Primary and Revision Total Hip Arthroplasty J. Bone Joint Surg. Am., Mar 2005; 87: 570 - 576. 4. The Epidemiology of Revision Total Hip Arthroplasty in the United States J. Bone Joint Surg. Am., Jan 2009; 91: 128 - 133. 5. Future Clinical and Economic Impact of Revision Total Hip and Knee Arthroplasty J. Bone Joint Surg. Am., Oct 2007; 89: 144 - 151. 6. Clinical Performance of Highly Cross-Linked Polyethylenes in Total Hip Arthroplasty J. Bone Joint Surg. Am., Dec 2007; 89: 2779 - 2786. 7. What Patient and Surgical Factors Contribute to Implant Wear and Osteolysis in Total Joint Arthroplasty? J. Am. Acad. Ortho. Surg., July 2008; 16: S7 - S13. 8. How Prevalent are Implant Wear and Osteolysis, and How Has The Scope of Osteolysis Changed Since 2000? J. Am. Acad. Ortho. Surg., July 2008; 16: S1 - S6. 9. What Other Biologic and Mechanical Factors Might Contribute To Osteolysis? J. Am. Acad. Ortho. Surg., July 2008; 16: S56 - S62. 10. Use of Antibiotic-Impregnated Cement in Total Joint Arthroplasty J. Am. Acad. Ortho. Surg., January/February 2003; 11: 38 - 47. 11. Dislocation After Total Hip Arthroplasty: Implant Design and Orientation J. Am. Acad. Ortho. Surg., March/April 2003; 11: 89 - 99. 12. Revision Total Hip Arthroplasty for Pelvic Discontinuity J. Bone Joint Surg. Am., Apr 2007; 89: 835 - 840. 13. How Have Alternative Bearings (Such as Metal-On-Metal, Highly Cross-Linked Polyethylene, and Ceramic-On-Ceramic) Affected The Prevention and Treatment of Osteolysis? J. Am. Acad. Ortho. Surg., July 2008; 16: S33 - S38. 14. How Do Alternative Bearing Surfaces Influence Wear Behavior? J. Am. Acad. Ortho. Surg., July 2008; 16: S86 - S93. REPRESENTATIVE CASES: Case 1 V.T., 54 y.o., female; underwent total hip arthroplasty with acetabular roof augmentation, right, for dysplastic hip, 12 years prior to revision; Patient presented with groin & thigh pain with shortening (3cm) of the right lower extremity. Pre-revision radiographs revealed aseptic loosening on both acetabular side & femoral side with proximal femoral bone loss. PRE-REVISION 3 YEARS POST-REVISION Patient underwent revision surgery using cementless acetabular (10mm offset cup) and femoral component (modular mid-length stem, fully coated) with 30mm calcar, 22mm head +10mm and proximal femoral cortical allograft. At three years post revision, the patient is ambulating without assistive device, functional range of motion on the right hip joint, no shortening and no pain. Radiographs revealed that the implants are in good alignment, no sign of loosening, migration or subsidence. Patient developed type 2 heterotopic ossification but did not affect the functional outcome. Case 2 N.M., 61 y.o., male; underwent cemented hemi-arthroplasty, right, 18 years prior to revision. Slipped and fell necessitating conversion to a cemented total hip. Sustained periprosthetic fracture and underwent revision hip surgery using a longer stem, a new acetabular cup cemented into the existing cup, and fibular strut graft. Patient developed infection 2 months after revision surgery. Patient presented with draining sinus, groin pain with shortening (4cm) of the right lower extremity. Pre-revision radiographs revealed protrusion of the endoprosthesis into the supero-medial wall of the left acetabulum. There’s also proximal femoral bone loss. Pre-revision radiographs revealed loosening on both acetabular side & femoral side. Patient underwent staged revision wherein the 1st stage entailed removal of all components and application of antibiotic spacer. Second stage involved removal of the antibiotic spacer and application of cementless acetabular (52mm) cup and femoral component (modular revision, curved stem, fully coated) with 30mm calcar, 28mm head +10mm and proximal femoral cortical allograft. At three years post revision, the patient is ambulating without assistive device, functional range of motion on the right hip joint, no shortening and no pain. Radiographs revealed that the implants are in good alignment, no sign of loosening, migration or subsidence. Patient developed type 2 heterotopic ossification but did not affect the functional outcome. INJURY FILM PRE-REVISION 1ST STAGE 3 YEARS POST 2ND STAGE