Whey: casein ratio in Infant Formula - does it matter?
advertisement

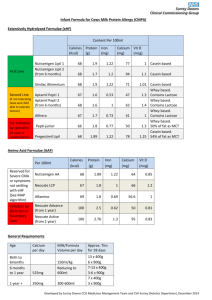
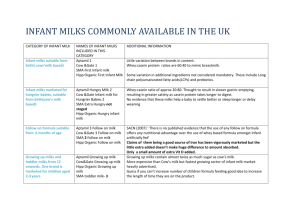
Hot Milk-February 2012 In this edition; Meeting the Mead Johnson rep page 1 Update on Infant Formula –Protein content page 1 Whey: casein ratio in Infant Formula - does it matter? Pages 2 and 3 Other evidence on protein in infant formula page 4 List of UK Infant Formula page page 4 Meeting the Mead Johnson rep Wednesday 25th April 10am-12 noon at NHS North Lancashire offices, Lancaster. This meeting is focussing on information about Mead Johnson specialist milks All staff are invited to this meeting. The meeting will last 2 hours - the start of the meeting will be to discuss information submitted by the rep, followed by the rep’s presentation. After the rep has left, the information will be reviewed and discussed and next steps agreed. We realise this is a significant commitment of time, but we want to encourage you (or a member of your team) to be involved in the appraisal process, and be part of the decision making process. Update on Infant Formula –Protein content In this Hot Milk we look at protein in Infant Formula. For more detail on this topic go to the excellent document produced by the Caroline Walker Trust, in particular Chapter 3 (page 23) and also page 40 in Chapter 4 Infant Milks in the UK 2011 CWT.pdf Report from the Infant Feeding Information Team, Blackpool and North Lancashire: February 2012 For further information contact infant.feeding@northlancs.nhs.uk 1 Whey: casein ratio in Infant Formula - does it matter? Key points; Breastmilk and cows milks have very different protein composition Cows milk is modified to try to imitate breastmilk We do not know if the modifications have the same effect. They may have a very different effect. Cows’ milk protein and soy protein are the main protein sources of most infant milks. Proteins are composed of many amino acids, eight of which cannot be made by the human body and so must be provided in adequate proportions in the diet. Protein requirements for infants are based on the concentrations of amino acids in mature human milk. The majority of infant formulas are based on highly modified cows’ milk. Both the protein quantity and protein composition differ between bovine milk and mature human milk. The total protein content of bovine milk is higher than that of mature human milk (3.3g/100ml vs. 1.3g/100ml respectively). Casein and whey are the two major proteins of human milk. Casein is the major protein source, and whey contains many different proteins and non-protein nitrogen. Colostrum is predominantly whey, and early breast milk is whey-dominant (60:40) but the proportions of casein and whey become approximately equal late in lactation. Whey and casein are present in bovine milk in different proportions to those found in breast milk, with casein the predominant protein source (whey: casein ratio typically 20:80). Human milk whey : casein ratios, which range from 90:10 initially to 50:50 in mature milk (12m+); but note that human milk proteins (whether whey or casein) are different from bovine milk proteins: there are differences in the function and make-up of the whey and casein in human milk and formula milk – for example cow milk protein has no lactoferrin, no immunoglobulin, no enzymes and far fewer of the non-protein nitrogen components. As Dr Judy Hopkinson, from the Baylor College of Medicine says, “The unique feature of human milk is that virtually every component examined plays some extra-nutritional role. The elegance of the system is remarkable – the more so the more we learn about it.” Artificial milk can have as much as 50% more protein than human milk. Protein intake pro rata to body weight is 55-80% higher in formula fed infants. High early protein intake enhances weight gain in infancy and can increase later obesity risk (Koletzko et al 2005) Report from the Infant Feeding Information Team, Blackpool and North Lancashire: February 2012 For further information contact infant.feeding@northlancs.nhs.uk 2 First infant formula has altered whey: casein ratio (60:40) to bring it closer to that found in breast milk which is whey-dominant. Formula aimed at ‘hungrier babies’ has a whey: casein ratio of 20:80 – similar to cows’ milks. “Hungry baby milks” are not currently recommended in the UK for young babies, even though manufacturer’s instructions on the tin say they are suitable from birth. IFIT have repeated current guidance in previous issues of Hot Milk, but here we explore why it might not be so simple: There has been an assumption, in guidance, that casein dominated milks are ‘worse’ than whey dominant milks as the whey dominant are the newer ones, but really independent comparative research is needed as to outcomes. Casein-dominant formulas were standard before filtration technology allowed whey residues from cheese-making to be processed to lower mineral content. Whey dominant came about because after environmental laws prevented the dumping of these by-products of cheese making, technology developed to mean that it could be used, while casein is useful for plastics, glue, paint and many other things. Current guidance and commentary implies that casein dominant milks are not suitable from birth, when actually the truth is we just don't know: it may be that some babies do better on casein dominants; indeed, one paper from the 1980’s showed that plasma amino acid profiles were better on casein dominant, (possibly because less protein was absorbed: casein molecules are bigger). Another possible difference is, as Lucas states, that casein hydrolysates are less antigenic than whey hydrolysates. And also now that overall protein levels in artificial infant milks are reduced, they may not provide enough protein - but until there's a comparative study we simply cannot know whether whey dominant is better than casein or vice versa. This study in the Cochrane library adds to the argument that there is no advantage to transfer a baby to casein based milks to help a baby feel full for longer (which is often why the switch happens); Similar gastric emptying rates for casein- and whey-predominant formulas in preterm infants. Thorkelsson et al (1994) http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/691/CN-00108691/frame.html Report from the Infant Feeding Information Team, Blackpool and North Lancashire: February 2012 For further information contact infant.feeding@northlancs.nhs.uk 3 Other evidence on protein in infant formula 1. This Cochrane review looks at protein levels for pre-term infants, Higher versus lower protein intake in formula-fed low birth weight infants, Sharisose et al (2009) http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003959.pub2/abstract “The ideal quantity of dietary protein for formula-fed low birth weight infants is still a matter of debate. Protein intake must be sufficient to achieve normal growth without negative effects such as acidosis, uremia, and elevated levels of circulating amino acids”. 2. Effect of taurine supplementation on growth and development in preterm or low birth weight infantsVerner el at (2009) http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006072.pub2/abstract “Despite that lack of evidence of benefit from randomised controlled trials, it is likely that taurine will continue to be added to formula milks and parenteral nutrition solutions used for feeding preterm and low birth weight infants given the putative association of taurine deficiency with various adverse outcomes. Further randomised controlled trials of taurine supplementation versus no supplementation in preterm or low birth weight infants are unlikely to be viewed as a research priority, but there may be issues related to dose or duration of supplementation in specific subgroups of infants that merit further research.” 3. Formulas containing hydrolysed protein for prevention of allergy and food intolerance in infants Osborn (2009) http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003664.pub3/abstract “There is no evidence to support feeding with a hydrolysed formula for the prevention of allergy compared to exclusive breast feeding. In high risk infants who are unable to be completely breast fed, there is limited evidence that prolonged feeding with a hydrolysed formula compared to a cow's milk formula reduces infant and childhood allergy and infant CMA. In view of methodological concerns and inconsistency of findings, further large, well designed trials comparing formulas containing partially hydrolysed whey, or extensively hydrolysed casein to cow's milk formulas are needed.” List of UK Infant Formula In last month’s Hot Milk we listed a number the most common brands being used. This was is not an exhaustive or infallible list so if you did spot a mistake or have some extra information please contact us. Report from the Infant Feeding Information Team, Blackpool and North Lancashire: February 2012 For further information contact infant.feeding@northlancs.nhs.uk 4