lecture_2015-03-101426002727127878904554ff1327abaa1
advertisement

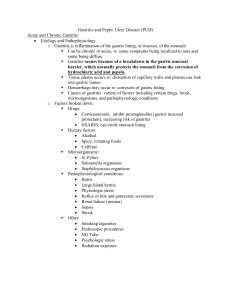
Gastrointestinal tract lab. I Chronic Peptic Ulcers Ulcer is a defect in the mucosa that penetrate at least into submucosa, and often into the muscularis propria or deeper. Chronic Lesion that occur in any portion of GIT exposed to the aggressive action of acidic peptic juices. 98% of peptic ulcers are either in the first portion of the duodenum or in the stomach, in a ratio of about 4:1. Causes 1. H. pylori infection. 2. Mucosal exposure to gastric acid & pepsin. Histopathological Findings (Microscopical features): Chronic peptic ulcers have 4 histologic zones (from within outside): 1. Necrotic zone lies in the floor of the ulcer. The tissue elements show coagulative necrosis giving eosinophilic smudgy appearance with nuclear debris. 2. Superficial exudative zone lies underneath the necrotic zone and is composed of fibrinous exudate containing necrotic debris and a few leucocytes, predominantly neutrophils. 3. Granulation tissue zone is seen merging into the necrotic zone. It is composed of nonspecific chronic inflammatory infiltrate and proliferating capillaries. 4. Zone of fibrosis is seen outer to the layer of granulation tissue and is composed of dense fibro-collagenic scar tissue. Clinical Features: 1. Epigastric pain. 2. Nausea & Vomiting. Complications: Bleeding. Perforation. Obstruction of the pyloric channel. Malignant transformation: Gastric and not duodenal. Gastrointestinal tract lab. I Gastric adenocarcinoma The most common malignant tumor of the stomach Risk Factors 1. Chronic Gastritis with intestinal metaplasia. 2. H. pylori infection. 3. Diets containing nitrites. 4. Decreased intake of fresh vegetables & fruits. 5. Partial gastrectomy. 6. Pernicious anemia. Classification According to Lauren classification Carcinoma of the stomach is divided into 2 types A. Intestinal type: arise from gastric mucous cells that undergo intestinal metaplasia in the setting of chronic gastritis & tend to be better differentiated. B. Diffuse type: arise denovo from Gastric mucous cells& is not associated with chronic gastritis & tends to be poorly differentiated. Gross appearance Exophytic: protrusion of the tumor mass into the lumen. Excavated: ulcerative lesion. Flat: with thickening of the wall of the stomach (linitis plastica) (in the diffuse type). Note: The lesser curvature is involved more the greater curvature. Microscopical appearance 1. The intestinal type is composed of malignant cells forming glands resembling colonic adenocarcinoma with different grades of differentiation, involving the mucosa & may extend to the muscularis properia. 2. The diffuse type is composed of mucous cells that penetrate the gastric wall as scattered individual (signet ring) cells (PAS positive).