Health Clinic Sub Folder (Sample)
advertisement
")
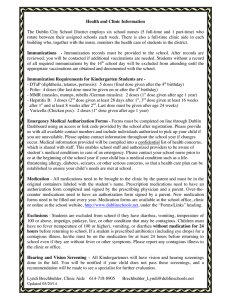
Health Clinic Sub Folder School Name Staff: Health Para: Office Secretary: Registrar: Principal: School Psych: District School Nurse: Contact Info: Health clinic: (phone #: Main office: (phone #: Office fax: (fax #: District Nurse: (phone #: School address: ) ) ) ) ***CONFIDENTIAL*** Health Clinic: Basics ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ - Follow treatment protocols for basic first aid in the health clinic o “Emergency Guidelines for Schools” (location: ) o Be sure to check student’s temperature with all “sick” visits; stomachache, HA, sore throat, etc. Follow Illness Policy - If a student injury is serious or a significant head injury (anything major), fill out: o Incident/Accident report (location: ) Keep report for District RN to review – do NOT put in student health folder or send home with student - Follow individual health care plans for students with medical needs o (location: ) o Only staff who have been trained and delegated by the RN may perform specific care procedures - Record all visits in the health clinic log (location: - Document all student visits in Powerschool o Student name, health, health office visits o Include: Chief complaint Observations (temp, etc) Treatment provided (rest, ice pack, etc.) Discharge (home/back to class, etc.) Discharge time ) Health Clinic: Daily Schedule 2014-2015 school year ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ 9:00 Student name - daily scheduled medication (name, dose) - treatment 11:30 Student name - daily scheduled treatment 12:00 Student name - medication (name, dose) 12:05 Diabetic student with pump - Check BG (supervise student check BG) - May give correction bolus before lunch (if BG is high) 12:40 Diabetic student with pump - Calculate grams of carbs eaten with student - Enter into insulin pump: carbs eaten, BG before lunch - Confirm insulin dosage and delivery - Record in IC: *Time, BG, carbs eaten, units of insulin administered 2:15 Student name - medication (name, dose) - treatment 3:20 Student name - medication (name, dose) - treatment Health Care Plans: 2014-2015 School Year The following students have Individual Health Care Plans – follow specific care procedures ***Trained and delegated staff only ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Student Name Grade *HCP’s are in a 3-ring binder, location: ( Meds? ) in the health clinic and must remain confidential *Diastat and Epi-Pens are located: ( )