Information Sheet for Clinic Visits
advertisement

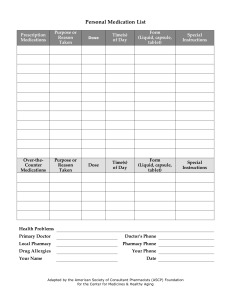
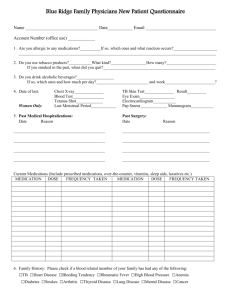
Information Sheet for Clinic Visits Your Name: Date of Birth: Today’s date: Primary Care Provider (Automatically receives our clinic note unless you tell us otherwise) Name: Address: Additional healthcare providers who should receive copies of the clinic note Name: Address: Name: Address: Medications: I take the following prescription medications Medication Size of pill, tablet, dose How many times a day I take the following non-prescription (over the counter) medications Medication Size of pill, How many times a day tablet, dose I take the following alternative or complementary medicine treatments Treatment Size of pill, tablet, dose How many times a day,week, month I am allergic to the following medications: Medication Questions or concerns for this visit: Nature of allergic reaction