Case investigation form - National Institute for Communicable
advertisement

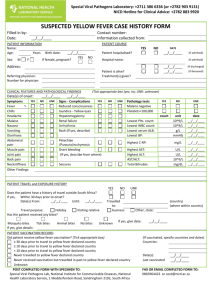
ARBOVIRUS Laboratory: +2711 386 6424/6391 (or +2782 903 9131) NICD Hotline for Clinical Advice: +2782 883 9920 SUSPECTED ARBOVIRUS CASE INVESTIGATION FORM Filled in by: Date: Contact number: Information collected from: __/__/____ DISEASE(S) UNDER INVESTIGATION (Tick appropriate boxes) Sindbis Chikungunya West Nile Dengue Rift Valley Other suspected clinical diagnoses: PATIENT INFORMATION Name: Age: Years Sex: M F Address: Other arbovirus: PATIENT COURSE YES Birth date: __/__/____ Patient hospitalised? Hospital name: Severity of illness? Treatment(s) given? Referring physician: Number for physician: NO DATE __/__/____ (If admitted) Mild __/__/____ (If discharged) Moderate Acute/Severe Consultation date: __/__/____ Px responsive to treatment? Not CLINICAL FEATURES Date of onset: __/__/____ And/or Duration illness: Main Syndrome: (Tick appropriate box) Fever without rash Fever with rash Arthritis and Rash Encephalitis/meningitis Retinitis/conjunctivitis Other remarkable symptoms: If present, Describe: Fever: Max Temp Rash (Site) face arm palms trunk legs soles Encephalitis Hemorrhage headache epitaxis °C neck stiffness haematemesis biphasic vomiting melaena constant confusion menorrhagia Duration (days): seizures petechiae unconscious purpura coma from venepuncture PATHOLOGICAL FINDINGS (Tick appropriate box (yes, no; UNK: unknown); Attach test results) YES NO UNK YES NO UNK Additional findings: Malaria negative Leucopenia Thrombocytopenia Lowest WBC count: 109/L Lowest plts count: 109/L Elevated liver function Latest plts. Count: 109/L Highest ALT: U/L Haematocrit: % Highest AST: U/L PATIENT EXPOSURE HISTORY Been diagnosed with dengue before? Been diagnosed with Rift Valley Fever before? Got Rift Valley Fever vaccination? Got Yellow Fever vaccination? Px occupation? During the past month, did patient travel? Rash (Appearance) macular papular petechial urticarial pruritic other YES NO UNK (If admitted) When? __/____ (month/year) __/____ (month/year) ____ (year) ____ (year) Since : ____ (year) From: Until: __/__/____ __/__/____ Less Well days Haemorrhagic fever Ocular disease pain inflammation blurred vision photophobia ↓visual acuity Where? Outdoors Another province Another country Name of place: Px had recent bites/unusual animal contact? __/____ (month/year) Mosquito bites Animal bite Animal blood/tissue Drank unpasteurized milk Tick bites Animal saliva Animal faeces/urine Consumed uncooked meat Other exposures: POST COMPLETED FORM WITH SPECIMEN TO: Special Viral Pathogens Lab, National Institute for Communicable Diseases, National FAX OR EMAIL COMPLETED FORM TO: Health Laboratory Service, 1 Modderfontein Road, Sandringham 2192, South Africa 0866671391 or cezd@nicd.ac.za