Case investigation form - National Institute for Communicable
advertisement

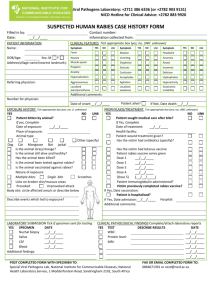
Special Viral Pathogens Laboratory: +2711 386 6336 (or +2782 903 9131) NICD Hotline for Clinical Advice: +2782 883 9920 SUSPECTED YELLOW FEVER CASE HISTORY FORM Filled in by: Date: __/__/____ PATIENT INFORMATION Name: Age: Years Sex: M Contact number: Information collected from: F PATIENT COURSE YES Birth date: __/__/____ If female, pregnant? YES NO NO Hospital name: Date(s) of onset: Symptoms °C Fever Chills Headache Malaise Nausea Vomiting Diarrhoea Abdominal pain Muscle pain Joint pain Back pain Neckstiffness YES __/__/____ __/__/____ Patient is alive? Treatment(s) given? Referring physician: Number for physician: __/__/____ NO UNK (If admitted) (If admitted) Address: CLINICAL FEATURES AND PATHOLOGICAL FINDINGS DATE __/__/____ Patient hospitalised? (If discharged) (If deceased) (Tick appropriate box (yes; no; UNK: unknown) __/__/____ Signs - Complications Reduced consciousness Jaundice - Yellow eyes Hepatomegalomy Renal failure Arrhythmia Rash (If yes, describe) YES NO UNK Pathology tests Malaria negative Platelets<100,000 YES NO UNK count unit 10^9/L 10^9/L g/L mmHG date __/__/____ __/__/____ __/__/____ __/__/____ Highest C-RP: mg/L __/__/____ Highest AST: Highest ALT: AST/ALT: Total Bilirubin: U/L U/L 10^9/L mg/dL __/__/____ __/__/____ __/__/____ __/__/____ Lowest Plts. count: Lowest WBC count: Lowest serum ALB: Lowest BP: Petechiae /Purpura/ecchymosis Overt bleeding (If yes, describe from where): Seizures Other Findings: PATIENT TRAVEL and EXPOSURE HISTORY YES Does the patient have a history of travel outside South Africa? If yes, Within 30 days prior to onset? Date(s) From: __/__/____ Until: __/__/____ Travel purpose: Holiday Has the patient received any bites? Mosquito bites Tick bites If yes, give details: Animal bites Visiting relative No bites NO UNK Travelled to: business Unknown (country) (where within country) Other, state: If yes, give date: PATIENT VACCINATION RECORD Did patient receive yellow fever vaccination? (Tick appropriate box) ≥ 30 days prior to travel to yellow fever declared country ≥ 10 days prior to travel to yellow fever declared country < 10 days prior to travel to yellow fever declared country Never travelled to yellow fever declared country Never received vaccination but travelled in past to yellow fever declared country Unknown POST COMPLETED FORM WITH SPECIMEN TO: Special Viral Pathogens Lab, National Institute for Communicable Diseases, National Health Laboratory Service, 1 Modderfontein Road, Sandringham 2192, South Africa __/__/____ (If vaccinated, specify countries and dates) Countries: Date(s): Last vaccinated __/__/____ __/__/____ FAX OR EMAIL COMPLETED FORM TO: 0865964423 or cezd@nicd.ac.za