Medical History
advertisement

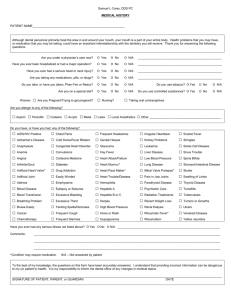
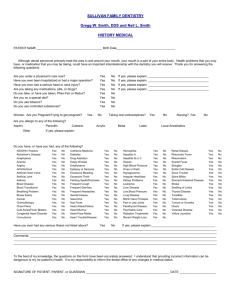
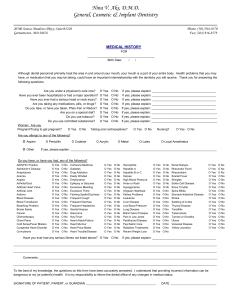
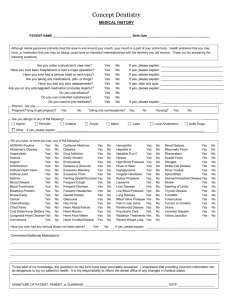
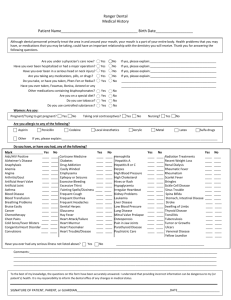
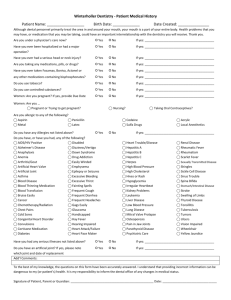
UNION FAMILY DENTAL CLINIC PATIENT NAME: SEX: PREFFERED NAME: DATE OF BIRTH: S.S.# PHONE NOS: (HOME): INSURANCE ID# (CELL): ADDRESS: APT/UNIT NO: CITY: PARENT/SPOUSE’S NAME: DOB: E-MAIL ADDRESS: (WORK): STATE: IN CASE OF EMERGENCY, WHO SHOULD BE NOTIFIED, BESIDES PERSON LISTED ABOVE? ZIPCODE: _________ PHONE NUMBER: WHOM MAY WE THANK FOR REFERRING YOU? FEMALES: ARE YOU PREGNANT OR TRYING TO GET PREGNANT? NAME OF OB/GYN DR: IF SO, DUE DATE: PHONE NO: ARE YOU NURSING? ARE YOU TAKING ORAL CONTRACEPTIVES? LIST ANY MEDICATIONS, NOTING REASON, DOSEAGE& FREQUENCY (USE SEPARATE PAGE IF TOO MANY TO LIST); HAVE YOU HAD MAJOR SURGERY OR BEEN HOSPITALIZED IN PAST FIVE YEARS? Reason/ Date: HAVE YOU EVER HAD A SERIOUS HEAD OR NECK INJURY? ARE YOU UNDER A PHYSICIAN’S CARE NOW: IF SO, PLEASE EXPLAIN: PHYSICIAN’S NAME/PHONE NUMBER: Are you allergic to any of the following? ASPIRIN: SULFA DRUGS: DATE OF LAST PHYSICAL EXAM: PENICILLIN: LOCAL ANESTHESIA: Does patient have, or has ever had, any of the following? YES NO AIDS/HIV POSITIVE □ □ CORISONE MEDICINE ALZHEIMER’S □ □ DIABETES ANAPHYLAX □ □ DRUG ADDICTION ANEMIA □ □ EASILY WINDED ANGINA □ □ EMPHYSEMA ARTHRITIS/GOUT □ □ EPILEPSY OR SEIZURES ART.HEART VALVE □ □ EXCESSIVE BLEEDING ARTIFICIAL JOINT □ □ EXCESSIVE THIRST ASTHMA □ □ FAINTING /DIZZINESS BLOOD DISEASE □ □ FREQUENT COUGH BLOOD TRANS □ □ FREQUENT DIARRHEA BREATHING PROBLEMS □ □ FREQUENT HEADACHE BRUISE EASILY □ □ GENITAL HERPES CANCER □ □ GLAUCOMA CHEMOTHERAPY □ □ HAY FEVER CHEST PAINS □ □ HEART ATTACK/FAILURE Cold Sore/Fever Blisters □ □ HEART MURMUR CONG.HEART DISORDER □ □ HEART PACEMAKER CONVULSIONS □ □ HEART TROUBLE/DISEASE CODEINE: ACRYLIC: LATEX: FOOD/OTHER ALLERGY: <explain> Does patient use tobacco products? □Yes □No YES NO HEMOPHELIA □ □ RADIATION TREATMENTS HEPATITIS A □ □ RECENT WEIGHT LOSS HEPATITIS B or C □ □ RENAL DIALYSIS HERPES □ □ RHEUMATIC FEVER HIGH BLOOD PRESSURE □ □ RHEUMATISM HIGH CHOLESTEROL □ □ SCARLET FEVER HIVES OR RASH □ □ SHINGLES HYPOGLYCEMIA □ □ SICKLE CELL DISEASE IRREGULAR HEARTBEAT □ □ SINUS TROUBLE KIDNEY PROBLEMS □ □ SPINA BIFADA LEUKEMIA □ □ STOMACH/INTEST DISEASE LIVER DISEASE □ □ STROKE LOW BLOOD PRESSURE □ □ SWELLING OF LIMBS LUNG DISEASE □ □ THYROID DISEASE MITRAL VALVE PROL □ □ TONSILLITIS OSTEOPOROSIS □ □ TUBERCULOSIS PAIN IN JAW JOINTS □ □ TUMORS OR GROWTHS PARATHYROID DISEASE □ □ ULCERS PSYCHIATRIC CARE □ □ VENEREAL DISEASE YELLOW JAUNDICE Has patient ever had or has any serious illness or conditions not listed above? □Yes □No If “yes”, please list: YES □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ NO □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ YES NO □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ ADDITIONAL INFORMATION/COMMENTS: TO THE BEST OF MY KNOWLEDGE, THE QUESTIONS ON THIS FORM HAVE BEEN ACCURATELY ANSWERED. I UNDERSTAND THAT PROVIDING INCORRECT INFORMATION CAN BE DANGEROUS TO MY (OR THE PATIENT’S) HEALTH: IT IS MY RESPONSIBLITY TO INFORM THE DENTAL OFFICE OF ANY CHANGES IN MEDICAL STATUS. SIGNATURE OF PATIENT,PARENT OR GUARDIAN: DATE: