Endoscopy Request Form (Opens in a new window)
advertisement
")
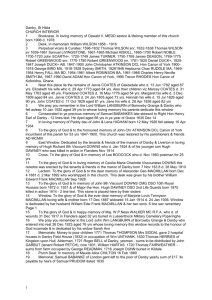
NHS e-Referral Service Endoscopy request form ALARM SYMPTOMS: Patient with any of these symptoms should be referred into appropriate 2WW service Dysphagia Epigastric mass Recent onset dyspepsia, aged >55 yrs Unintentional weight loss Persistent vomiting Iron deficiency anaemia with no obvious cause Obstructive jaundice PR bleeding persistently, without loose stools and without anal symptoms, aged >50 yrs PR bleeding & loose / more frequent stools for > 6 wks Loose/more frequent stools > 6 weeks, aged > 50 yrs Right sided mass Rectal mass SECTION 1: PATIENT DEMOGRAPHIC DETAILS Patient NHS number: UBRN: Patient first name: Patient last name: Date of Birth (DD/MM/YY): Gender: Male Female st Patient address (1 line): Patient town / city: Patient postcode: Patient contact number: Patient contact number 2: SECTION 2: REFERRER INFORMATION First name: Last name: Referrer role: GP Other GP Practice Code: Referrer contact no: GMC registration number: Referrer e-mail address: INDICATIONS FOR AN ENDOSCOPY: Gastroscopy Flexible Sigmoidoscopy Change in bowel habit, no rectal bleeding, aged < 50 yrs Painless rectal bleeding, aged < 50 yrs Peri-anal symptoms, any age Recent onset of reflux symptoms that fails to respond to PPI and/or gastro prokinetic therapy Positive helicobacter test & dyspepsia that fails to respond to eradication therapy Dyspepsia and concurrent use of NSAIDs For duodenal biopsy – indications are iron deficiency anaemia, diarrhoea, unexplained weight loss and positive coeliac serology. Consider 2WW for alarm symptoms. SECTION 3: INVESTIGATION REQUEST DETAILS Current Request Gastroscopy (Upper GI) Please complete Section 4 and 5 Flexi Sigmoidoscopy (Lower GI) Please complete Section 4 Colonic Imaging Advice (CIA) Please complete Section 4 and 5 Patient had previous endoscopy? Yes If yes, what type of previous endoscopy? Gastroscopy UBRN: Reason for request: Relevant clinical history: No Date (DD/MM/YYYY): Flexi Sigmoidoscopy Colonoscopy SECTION 4: MEDICAL INFORMATION (all requests) Is the patient fit for a day case procedure? Yes If unsure refer patient to relevant outpatient clinic and not for direct access Note: If the patient requires sedation, they must be able to organise an escort home and have observation overnight Does the patient have capacity to give informed consent? Is this patient diabetic? Yes No Yes No If yes, is the patient insulin dependent? Yes No Has the patient had poorly controlled angina / MI in last 3 months? Yes No Has the patient had prosthetic valve replacement? Yes No Has the patient previously had subacute bacterial endocarditis? Yes No Has the patient had a vascular graft within the last year? Yes No Does the patient have COPD / poorly controlled asthma? Yes No Is the patient on Warfarin? Yes No Duration: Yes No Which Drug? Is the patient on aspirin, clopidogrel, or any other anti-platelet drug? Duration: If you have answered ‘yes’ to any of the questions above, please ensure that you include any additional relevant clinical information above. SECTION 5: GASTROSCOPY AND CIA ONLY H Pylori status: Positive Negative Not known NSAID: Yes No Duration (weeks): Must continue: PPI/H2 antagonist: Yes No Duration (weeks): Patient responded Yes Yes No No