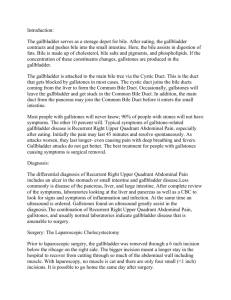
Fig. 1-8 Lobes of the liver (Ghimire 2013)
advertisement
")
Bachelor in Medical Imaging Faculty of Health Sciences Puncak Alam Campus INVESTIGATION OF HEPATOBILIARY SYSTEM ABNORMALITIES COURSE NAME SPECIAL RADIOGRAPHIC PROCEDURE 1 COURSE CODE MRD551 STUDENT NAME MOHD AMIR SYAHMI BIN MAT RAZALI STUDENT NUMBER 2013226136 COURSE LECTURER DR. MOHD HANAFI ALI Due Date: 09 DECEMBER 2013 Date of Submission: 09 DECEMBER 2013 1 TABLE OF CONTENT INVESTIGATION OF HEPATOBILIARY SYSTEM ABNORMALITIES NO 1 2 3 4 5 6 7 8 9 10 11 12 TOPIC / SUBTOPIC COVER PAGE TABLE OF CONTENT LIST OF TABLE AND FIGURES INTRODUCTION RADIOGRAPHIC ANATOMY OF HEPATOBILIARY SYSTEM TERMINOLOGY IN HEPATOBILIARY SYSTEM HEPATOBILIARY SYSTEM ABNORMALITIES GALLBLADDER AND BILIARY DUCTS RADIOGRAPHY RADIOGRAPHIC POSITIONING IN HEPATOBILIARY SYSTEM PROCEDURE CONCLUSION REFFERENCES ASSIGNMENT SUBMISSION FORM PAGE 1 2 3 4-5 6-14 15-16 17-19 20-33 34-47 48-49 50 51 2 LIST OF TABLES AND FIGURES 1. Table 1-1 Terminalogy In Hepatobiliary System (Bontrager & Lampignano 2005, p. 529) (Page – 16) 2. Table 1-2 Summary Table Of Gallbladder And Biliary System Procedures (Bontrager & Lampignano 2005, p. 536) (Page – 33) 3. Fig. 1-1 Topographic of the liver (RH – Right Hypogastrum, EG – Epigastrium, LH – Left Epigastrium, RL – Right Lumbar Region, U – Umbilical Region, LL – Left Lumbar region, RI Right Iliac Fossa, HG – Hypogastrium and LI – Left Iliac Fossa) (Ghimire 2013) (Page – 7) 4. Fig. 1-2 Liver in-situ (anterior thoracic and abdominal walls removed) (Ghimire 2013) (Page – 7) 5. Fig. 1-3 Relation of the Liver. Left Top – Superior view. Right Top – Posterior View. Left Bottom – Anterior View and Right Bottom – Inferior View. (Ghimire 2013) (Page – 8) 6. Fig. 1-4 Surfaces of the Liver. Left Top – Superior view showing most of the superior surface. Right Top – Posterior View – Posterior and inferior surface of the liver are seen. Left Bottom – Anterior View – Superior, anterior and part of the right surfaces are seen and Right Bottom – inferior View, inferior and posterior surfaces are seen. (Ghimire 2013) (Page – 9) 7. Fig. 1-5 Ligament of the Liver. Note the ligamentum teres enclosed in the free margin of falciform ligament. Anterosuperior View. (Ghimire 2013) (Page – 9) 8. Fig. 1-6 Ligament of the Liver. Also note the ‘bare area’ of the liver – Posterosuperior View. (Ghimire 2013) (Page – 10) 9. Fig. 1-7 Ligament of the Liver. Posteroinferior View. (Ghimire 2013) (Page – 10) 10. Fig. 1-8 Lobes of the liver (Ghimire 2013) (Page – 11) 11. Fig. 1-9 Ducts of the Liver. (Underlined with red lines). (Ghimire 2013) (Page – 12) 12. Fig. 2 Body Habitus And Gallbladder Location. (Gallbladder body habitus n.d.) (Page – 14) 13. Fig. 2-1 Patient Positioning Left Anterior Oblique (Meschan 1955) (Page – 24) 14. Fig. 2-2 T-Tube Placement In Surgery (Polaski & Tatro 1996) (Page – 27) 15. Fig. 2-3 PTC Procedure (Chapman & Nakielny n.d.) (Page – 30) 16. Fig. 2-4 ERCP Procedure (ERCP n.d.) (Page – 31) 17. Fig. 2-5 Radiographic Positioning – Gallbladder (PA) (Chunggjaa 2010) (Page – 37) 18. Fig. 2-6 Left Anterior Oblique – Gallbladder (LAO) (Chunggjaa 2010) (Page – 41) 19. Fig. 2-7 Right Lateral Decubitus (PA) – Gallbladder (Chunggjaa 2010) (Page – 44) 3 4 INTRODUCTION In this assignment, the information about investigation of hepatobiliary system abnormalities will be explained. There are many ways to investigate the abnormalities of hepatobiliary system but i will be focusing more on plain radiographic examination and fluoroscopic examination aided with contrast media. Firstly, I will go through to the anatomy and physiology of hepatobiliary system. As we know, the hepatobiliary system consists of several organs which are liver, gallbladder, bile ducts, and pancreas. In this topic, it will contain the explanation about the structure and function of each organ in hepatobiliary system. In the subtopic of radiographic anatomy of hepatobiliary system, I will explain more about the location of the gallbladder based on patient’s body habitus. Then I will go through to the terminology that commonly used in hepatobiliary system. As a radiographer, one should know all the terms because it will help us more on understanding the anatomy, pathology or the procedures of hepatobiliary system. Besides that, I will also explain briefly about the abnormalities or pathology of the hepatobiliary system. There are a lot of abnormalities in hepatobiliary system, but I will be focusing more on the abnormalities which usually happened in hepatobiliary system such as biliary calculi, cholecystisis, biliary stenosis and neoplasm of the hepatobiliary system. Lastly, I will go through to the radiographic examination of hepatobiliary system. In this subtopic, I will explain more about each procedure of hepatobiliary system whether it is fluoroscopic studies or conventional radiographic studies. It contain the patient’s preparation of the procedure, the techniques used in each examination, and the radiographic images criteria for each examination. 5 6 RADIOGRAPHIC ANATOMY OF HEPATOBILIARY SYSTEM Liver Location And Anatomy Structure Fig. 1-1 Topographic of the liver (RH – Right Hypogastrum, EG – Epigastrium, LH – Left Epigastrium, RL – Right Lumbar Region, U – Umbilical Region, LL – Left Lumbar region, RI Right Iliac Fossa, HG – Hypogastrium and LI – Left Iliac Fossa) (Ghimire 2013) Fig. 1-2 Liver in-situ (anterior thoracic and abdominal walls removed) (Ghimire 2013) 7 The hepatobiliary system consist of liver, gallbladder, bile ducts and pancreas. Knowledge of basic anatomy and physiology of liver, gallbladder and connecting ducts are important to understand more about its radiographic examination. The liver is the biggest organ in human body which occupied most of the right upper quadrant of the abdominal region. Most of the liver structure located in right hypochondrium and epigastrium. Left hypochondrium is the part that less occupied by the liver. It also has triangle-shaped physical and weighs about 3-4 pounds or 1.5 kilogram in normal human body. As viewed from anteroposterior aspect, the superior border of the liver is the widest part which is convex to conform to the inferior surfave of the right hemidiaphragm. The liver has the biggest vertical dimension at it’s right border where it extends above the right kidney, slightly inferior to the lateral portion of the tenth rib. The lower right rib cage is very important because it will protect the liver from trauma and other harmful physical impact. (Bontrager & Lampignano 2005, p. 526) Fig. 1-3 Relation of the Liver. Left Top – Superior view. Right Top – Posterior View. Left Bottom – Anterior View and Right Bottom – Inferior View. (Ghimire 2013) 8 Fig. 1-4 Surfaces of the Liver. Left Top – Superior view showing most of the superior surface. Right Top – Posterior View – Posterior and inferior surface of the liver are seen. Left Bottom – Anterior View – Superior, anterior and part of the right surfaces are seen and Right Bottom – inferior View, inferior and posterior surfaces are seen. (Ghimire 2013) Fig. 1-5 Ligament of the Liver. Note the ligamentum teres enclosed in the free margin of falciform ligament. Anterosuperior View. (Ghimire 2013) 9 Fig. 1-6 Ligament of the Liver. Also note the ‘bare area’ of the liver – Posterosuperior View. (Ghimire 2013) Fig. 1-7 Ligament of the Liver. Posteroinferior View. (Ghimire 2013) 10 Fig. 1-8 Lobes of the liver (Ghimire 2013) Normally, the liver is divided into two major and two minor lobes. In anteroposterior aspect, only two major lobes can be seen. Falciform ligament separate the larger right lobe and the smaller left lobe. The large right lobe divide into two minor lobes (quadrate lobe and caudate lobe) which only can be seen in inferior and posterior view. The liver is an organ that is very important to human body. It gives a lot of benefits to human body but the main function applicable to radiographic examination is to produce large amounts of bile. This bile will help the digestion and absorption of fats in human body. Besides that, liver also will remove any potentially harmful toxic which are obtained from our daily foods. Other functions of the liver are to (regulate blood glucose and lipids), (keep certain micronutrients, iron and vitamins) and (provides thermal energy to body especially at rest). (Bontrager & Lampignano 2005, p. 526) 11 Gallbladder And Biliary Ducts Fig. 1-9 Ducts of the Liver. (Underlined with red lines). (Ghimire 2013) 12 Gallbladder And Biliary Ducts Located outside of the liver are the extrahepatic biliary ducts and the gallbladder. The production of bile are located in small lobules of the liver. Then, it will travel through either the right and left hepatic duct and will join to the common hepatic duct. For temporary storage, the bile will be carried to the gallbladder or it will be secreted into the duodenum through the common bile duct which is joined by the main pancreatic duct. The physical appearance of gallbladder looks like a pear-shaped sac and normally from 7 to 10 centimeters long.The gallbladder is divided into three main parts which are fundus, body and neck. As we knows, the gallbladder has three main functions to our body. Firstly, it will be the storage of the bile that are no needed for digestive process. Second function of the gallbladder is to concentrate the bile due to hydrolysis. The last known function of the gallbladder is to contract especially when the foods that contain fatty acids or fats exist in the duodenum. This contraction happened due to the secretion of cholecystokinin hormone (CCK) from the duodenal mucosa which are stimulated by that type of foods. The common bile duct usually located behind the superior portion of the duodenum and it usually about 7.5 centimeters in length. It also has an internal diameter about the size of a drinking straw. The end of the pancreatic duct (duct of Wirsung) is firmly conjoined with the end of the common bile duct. Some people have the condition where their common bile duct joins the pancreatic duct to form one path through the single papilla into the duodenum while some others have them separated. That path or passageway known as ampulla of Vater or hepatopancreatic ampulla. Sphincter of Oddi or the hepatopancreatic ampulla is a circular muscle fiber which is located near to the terminal opening of the ampulla of Vater into the duodenum. (Bontrager & Lampignano 2005, p. 527) Gallbladder And Biliary Ducts (Lateral View) In lateral view of the abdomen, the gallbladder can be seen anterior to the midcoronal plane and the duct system is located midway between the posterior and the anterior part of the human body. In imaging technique, it is important to locate the gallbladder as close to the image receptor as possible to have the best projection of its structure. Then, the prone position will be much greater than the supine position. (Bontrager & Lampignano 2005, p. 528) 13 Body Habitus And Gallbladder Location Fig. 2 Body Habitus And Gallbladder Location. (Gallbladder body habitus n.d.) The common position of the gallbladder are different depends on the body build of the patient / human. The gallbladder normally located superiorly and more lateral than usual in hypersthenic body habitus. Then, the best positioning of this type of body habitus is Left Anterior Oblique (LAO) which is slightly oblique rotation of 15̊ to 20̊ . Whereas for the average body habitus (sthenic and hyposthenic types), 20̊ to 25̊ LAO position is need to move the gallbladder away from the spine. This is because the gallbladder is located about midway between the lower lateral rib margin and the xiphoid tip. While for the asthenic body habitus, the gallbladder is located near to the level of iliac crest and the midline of the human body. To project the gallbladder away from the spine, a 35̊ to 40̊ rotation of LAO positioning is needed. (Bontrager & Lampignano 2005, p. 528) 14 15 TERMINOLOGY IN HEPATOBILIARY SYSTEM TERM MEANING Chole Prefix denoting relationship to bie Cysto Prefix denoting sac or bladder Cholecystogram Radiographic examination of the gallbladder Cholangiogram Radiographic examination of the biliary ducts Cholecystocholangiogram Study of both the gallbladder and biliary ducts Choleliths Gallstones Cholelithiasis Condition of having gallstones Cholecystisis Inflammation of the gallbladder Cholecystectomy Surgical removal of the gallbladder PTC Percutaneous Transhepatic Cholangiogram ERCP Endoscopic Retrograde Cholangiopancreatography Table 1-1 Terminalogy In Hepatobiliary System (Bontrager & Lampignano 2005, p. 529) 16 17 HEPATOBILIARY SYSTEM ABNORMALITIES (PATHOLOGIC INDICATIONS) Biliary Calculi Existence of abnormal calcifications or stones in the gallbladder is cholelithiasis. During OCG, it is common to diagnosed the abnormality like cholelithiasis. The formation of the gallstones are caused by increasing level of cholesterol, calcium or bilirubin. The higher percentage of peoples to have gallstones are female and obese patients. Right upper quadrant pain commonly after meal, vomiting and nausea are the symptoms of cholelithiasis. Emulsion of biliary stones in the gallbladder is milk calcium bile. It is hard to diagnose during OCG this emulsion buildup of calcium deposits within the gallbladder. PA scout image is the best way to project this milk calcium as it will seen as a diffuse collection of sand-like calcifications or sediment. Presence of the stones in the biliary ducts is Choledocholithiasis. Biliary stones may build in the biliary ducts or move from the gallbladder. Blockage in the ducts is usually produced by these stones. Pancreatitis, jaundice, pain and tenderness in the right upper quadrant of the abdomen are the symptoms of the gallbladder and biliary disease. (Bontrager & Lampignano 2005, p. 530) Cholecystisis Inflammation of the gallbladder whether it is acute or chronic is cholecystisis. Commonly, blockage of the cystic duct restrict the flow of bile from the gallbladder into the common bile duct produced by acute cholecystisis. This is because a stone lodged in the neck of the gallbladder. After some time, the bile begins to irritate the inner lining of the gallbladder and it becomes inflamed. Fever, tenderness in the right upper quadrant of the abdomen and abdominal pain are the symptoms of acute cholecystisis. It may also produce by bacterial infection and ischemia. During OCG, it is hard to see gallbladder with acute cholecystisis become radiopaque. (Bontrager & Lampignano 2005, p. 530) Chronic cholecystisis usually connected with gallstones but may also be an outcome of carcinoma of the gallbladder or pancreatitis. Heartburn, nausea after the meal and right upper quadrant of abdominal pain are the symptoms of chronic cholecystisis. It may also attacks 18 repetitively after meals normally subside in 1 to 4 hours. Thickening or calcification of the wall of the gallbladder can also be connected to this disease. (Bontrager & Lampignano 2005, p. 530) Neoplasm New growths, whether it is benign or malignant is called neoplasms. Cancerous tumor of the gallbladder which is aggressive and may spread to another organs such as pancreas, liver and GIT tract is called Malignant. Cholesterol polyps and adenomas are the common benign tumor of the gallbladder. Most of the patients who have carcinoma of the gallbladder may have the gallstones. This happened because the growth of the tumors may obstruct the biliary system and patients may have the symptoms such as jaundice, pain and vomiting. (Bontrager & Lampignano 2005, p. 530) Biliary Stenosis It can be defined as narrowing of one of the biliary ducts and may reduce the flow of the bile. Obstruction of the ducts may happen due to stenosis which it prevent the passage of the gallstones into the duodenum. Biliary stenosis may also resulted by jaundice or cholecystisis. The common bile duct will seen elongated, narrow and tapered in cholangiography. A gallstone usually may seen collected at distal common bile duct and common presents a filling defect with a small portion of contrast media around it. (Bontrager & Lampignano 2005, p. 530) Congenital Anomalies Abnormalities of the gallbladder which the patient have since birth are call congenital anomalies of the gallbladder. Commonly, most of them are benign and may affect the biliary system in aspect of production, storage and release of the biles. (Bontrager & Lampignano 2005, p. 530) 19 20 Oral cholecystogram Abbreviated as OCG, oral cholecystogram is a procedure which contrast media is ingested orally. Four to six tablets or capsules are ingested during the evening preceding the OCG examination. Visualization of gallbladder aided by oral contrast media termed as cholecystopaques. (Bontrager & Lampignano 2005, p. 529) Purpose To exam radiographically the anatomy and function of the biliary system is the main purpose of the oral cholecystogram. Other purposes are; 1. To measure the functional ability of the liver to remove the orally administered contrast medium from the bloodstream and to excrete it along with the bile. 2. The condition and patency of the biliary ducts. 3. The contracting and concentrating ability of the gallbladder. (Bontrager & Lampignano 2005, p. 529) Contraindications 1. Active gastrointestinal disease (vomiting & diarrhea). 2. Chronic hepatorenal disease, especially with renal impairment (acute or chronic liver failure, renal failure and sever jaundice). 3. Pregnancy. 4. Allergic reactions to iodine-containing compounds. (Bontrager & Lampignano 2005, p. 529) 21 Oral Cholecystogram Procedure Patient Preparation It has well correlation with examination preparations for an upper GI series. So, both of them are usually scheduled on the same morning. 1 or 2 days before the gallbladder examination, some fat diet must be taken by the patient to exam the functional contraction of the gallbladder due to the ingestion of the fats. The gallbladder has to be emptied before the introduction of contrast medium. When the contrast medium is administrated and with the newly formed bile, it is a greater chance it will be stored in the gallbladder. During the 24-hour before the examination, laxatives must to be avoided. The patients must have light evening meal which contain free-fat foods. The patients also must fast at least 8 hours before the examination and did not chew the chewing gum and smoke until after the exam is finish if the OCG procedure is combined with an upper GI study. Usually, the patient must take 4 to 6 tablets or capsules after the evening meal before 9 p.m but it depends on the type of the contrast medium used. Cholecystopaques are usually most effective if it was taken 10 to 12 hours before the examination. The patient must come to the hospital early in the morning and no breakfast is allowed. When they arrive in the radiology department for OCG procedure, they will be instructed by the radiographer to remove all clothing from chest and abdomen areas and wear a hospital gown. (Bontrager & Lampignano 2005, p. 531) 22 Patient Interview Patient has to be questioned about taking the contrast medium before the scout radiograph is taken. It is important to know precisely at what time and how many pills were taken by the patient. Radiographer must also confirm the pills or capsules that are taken by the patient are the right ones. Besides that, any anaphylactoid or allergic reactions must be noted by asking the patient regarding any reactions that they may have after taking the pills or capsules. Examples of the allergic reactions of contrast medium are nausea, vomiting or diarrhea. It also important to confirm that patients have not taken their breakfast in the morning before the examination and they still have the gallbladder. It is not relevant to do OCG procedure to the patients who have already removed their gallbladder surgically. Lastly, it is a must to question the female patient whether she is pregnant or not as a precautions for high radiation abdominal radiographic exams. (Bontrager & Lampignano 2005, p. 531) Imaging Routine To exam the presence or absence of an opacified gallbladder, a scout radiograph must be taken first on 14 x 17 inches (35 x 43 cm) or 10 x 12 inches (24 x 30 cm) image receptor (IR) at 70 to 80 KvP. (Bontrager & Lampignano 2005, p. 531) The radiographer or the technologist must determine 4 aspects if the gallbladder shadow is present in scout radiograph : 1. The exact location of the gallbladder. 2. Any presence that overlap the gallbladder whether it is intestine or bone. 3. Concentration of contrast medium for other additional imaging studies. 4. The optimal exposure factors of the gallbladder imaging. (Bontrager & Lampignano 2005, p. 531) 23 LAO And Right Lateral Decubitus (PA) Or Erect PA In OCG procedure, the Left Anterior Oblique is a common imaging routin, in addition to either an erect PA or a right lateral decubitus projection. To stratify the gallstones and to allow the gallbladder to assume a different position in the abdominal cavity in relationship to the spine or other abdominal structures, an erect or the lateral decubitus position is an important projection. Optimally visualization of the gallbladder can be obtain by fluoroscopy and spot imaging as it permits use of compression and small positional changes. (Bontrager & Lampignano 2005, p. 531) Fig. 2-1 Patient Positioning Left Anterior Oblique (Meschan 1955) 24 Special Radiographic Biliary Duct Procedure And Pathologic Indications Operative Cholangiogram 1. The primary purpose is to reveal any choleliths not previously detected. 2. Investigate the patency of the biliary tract. 3. Demonstrate small lesions, stricture, or dilations within the biliary. 4. Determine the functional status of the papilla of Vater. (Bontrager & Lampignano 2005, p. 532) Posteperative T-Tube Chilangiogram 1. Evaluate the status of biliary system. 2. Visualize any residual undetected choleliths. 3. Extract small stone from biliary duct during the T-tube procedure using a special basket catheter. 4. Demonstrate small lesions, strictures, or dilations in the biliary ducts. (Bontrager & Lampignano 2005, p. 532) Percutaneous Transhepatic Cholangiography (PTC) 1. Biliary drainage and stone extraction: a. Using the special equipment, radiologist could diagnose and remove the stone or dilate the restricted portion of the biliary tract. To decompress the biliary ducts, excess bile may be drained during PTC procedure. 2. Obstructive jaundice: a. The ducts are suspected to be dilated if the patient is jaundiced due to obstruction of the biliary duct (biliary stenosis or calculi). (Bontrager & Lampignano 2005, p. 532) 25 Endoscopic Retrograde Cholangiopancreatography (ERCP) 1. Demonstrate small lesions, dilations, or stricture within the biliary/pancreatic ducts. 2. Investigate the patency of the biliary/pancreatic ducts. 3. Reveal any choleliths not previously detected. (Bontrager & Lampignano 2005, p. 532) 26 Operative (Immediate) Cholangiogram This procedure is usually performed during surgery or during cholecystectomy where the surgeon removes the gallbladder. After the gallbladder is removed due to the residual stones that are suspected and located in one of the biliary ducts, a small catheter is inserted into the remaining portion of the cystic duct. Radiographic images are obtained when iodinated contrast media is administered. (Bontrager & Lampignano 2005, p. 533) Postoperative (T-Tube Or Delayed) Cholangiography This postoperative procedure also known as delayed cholangiography or T-tube. After cholecystectomy procedure, postoperative cholangiography commonly performed in the radiology department. During the surgery, the residual stones in the biliary ducts that went undetected maybe concerned by the surgeon. T-tube catheter will be inserted into the common bile duct by the surgeon during the cholecystectomy if the concern about the residual stones are existed. The catheter extends to the outside of the body and is clamped off. (Bontrager & Lampignano 2005, p. 533) Fig. 2-2 T-Tube Placement In Surgery (Polaski & Tatro 1996) 27 Summary Of Postoperative (T-Tube) Cholangiography Procedure Fluoroscopic suite must be prepared and the set up of the examination tray must be in complete. Contrast media must be selected and prepared based on patient’s condition whether the patient have the allergic reactions to iodinated contrast media or not. Appropriate scout images must be taken to verify the position and technique of the procedure. Patient’s condition must always be monitored during the procedure. Conventional radiograph must be produce if it is requested by the radiologist. The iodinated contrast media is injected fractionally and fluoro spot films are taken after the duct drainage under fluoroscopic control. While injecting the contrast media, it is important to make sure there is no air bubbles administered because it may be confused for radiolucent stones. The radiologist may elect to remove them if residual stones are detected. A basket may be passed over a guide wire and the stones will be removed. (Bontrager & Lampignano 2005, p. 533) Percutaneous Transhepatic Cholangiography (PTC) Another type of cholangiography that demonstrates the biliary duct is known as PTC. It is less frequently performed because it is more invasive than other forms of cholangiography. This procedure involves a direct pucture of biliary ducts with a needle passing through the liver. Iodinated contrast media is administered, once the needle is within a duct under fluoroscopic control. Conventional radiographic images and fluoroscopic spot images are taken during the procedure. (Bontrager & Lampignano 2005, p. 534) 28 Procedure There are 3 major risks associated with the PTC because of the needle puncture into the liver tissues. 1. Pneumothorax : The needle puncture may result in pneumothorax because the liver is near the right hemidiaphragm. A chest radiograph may be ordered after the procedure if pneumothorax is suspected. 2. Liver hemorrhage : The liver may hemorrhage internally, or bile may escape into the peritoneal cavity. 3. Escape of bile : Inflammation of surrounding tissue due to escape of the bile into the peritoneal cavity. PTC also serve as therapeutic procedure as it extract or decompress dilated ducts. (Bontrager & Lampignano 2005, p. 534) The patient’s vital signs are closely monitored during and after the procedure to detect deterioration. The site of puncture is surgically prepared. The radiologist inserts the needle into the liver in the approximate location of the biliary ducts, after the local anesthetic is given. More than one puncture may be necessary to locate the appropriate duct. The radiologist adjusts the needle while slowly injecting the contrast media under fluoroscopic view. Fluoroscopic spot image and conventional radiographic images are taken once the ducts are filled. A larger needle may be inserted into a duct containing a stone. A special basket or loop catheter is passed over a guide wire and is positioned near the stone. The stone can be extracted from the duct under the fluoroscopic control. (Bontrager & Lampignano 2005, p. 534) Summary Of PTC Procedure The technologist has specific responsibilities although the percutaneous transhepatic puncture is performed by the radiologist. Fluoroscopic suite must be prepared and set up for the sterile tray including the long, thin-walled needle use for the puncture must be done. Chiba or skinny needle has a flexible shaft that allows for easy manipulation of the needle during the procedure. Contrast media must be prepare to determine whether the patients have hypersensitivity to iodionated 29 contrast media or not. Those persons remaining in the room during the exposure must be provided with lead aprons. To verify position and technique, appropriate scout images must be taken. Patients must be always monitored during the procedure. Chest radiographic image are taken following procedure if requested by radiologist. (Bontrager & Lampignano 2005, p. 534) Fig. 2-3 PTC Procedure (Chapman & Nakielny n.d.) 30 Endoscopic Retrograde Cholangiopancreatography (ERCP) ERCP is another examination of the biliary and main pancreatic ducts and that is performed more frequently. (Bontrager & Lampignano 2005, p. 535) Endoscopy Endoscope is an instrument that allows illumination of the internal lining of a organ while endoscopy is inspection of any cavity of the body. To examine the interior lining of the stomach, duodenum and colon, various fiber-optic endoscopes are available to use. Older types of endoscopes allow for individual viewing only through an eyepiece, but newer video endoscopes project the image onto the video monitors for multiple viewing. Duodenoscope, also a special type of fiber-optic endoscope is commonly used for ERCP procedure. It provides a wide angle side view when inserted into the duodenum through the mouth, esophagus, and stomach for locating and inserting a catheter or cannula into the small opening of the sphincter of Oddi, leading from the duodenum into the common bile duct and the main pancreatic ducts. (Bontrager & Lampignano 2005, p. 535) Fig. 2-4 ERCP Procedure (ERCP n.d.) 31 Diagnostic Or Therapeutic ERCP can be performed to relieve certain pathologic conditions therapeutically. This can be either to repair a stenosis of the hepatopancreatic sphincter or to remove choleliths or small lesions. Insertion endoscopically of catheter or injection cannula into the common bile duct or main pancreatic duct under fluoroscopic control, followed by retrograde injection of contrast media into biliary duct is the diagnostic role of ERCP. The conclusion is the ERCP can be either a diagnostic or a therapeutic procedure. (Bontrager & Lampignano 2005, p. 535) Summary Of ERCP Procedure Fluoroscopic suite must be prepared and the set up for the examination tray must be in complete. Contrast media must be selected and prepared based on patient’s condition whether the patient have the allergic reactions to iodinated contrast media or not. Appropriate scout images must be taken to verify the position and technique of the procedure. For the placement of the catheter or injection cannula, gastroenterologist must be assisted with fluoroscopy. Patient must be always monitored during the procedure. Conventional radiographic image are produced as requested by radiologist. (Bontrager & Lampignano 2005, p. 535) Precautions The patient should remain NPO for at least 1 hour after the procedure due to the patient’s throat is anesthetized during the procedure. This will prevent aspiration of food or liquid into the lungs. The clinical history of the patient must be reviewed to determine whether the patient has pancreatitis or a pseudocyst of the pancreas. Injecting contrast media into a pseudocyst may lead to a rupture. Radiographers must always ensure that all persons in the fluoroscopy room wear protective aprons. (Bontrager & Lampignano 2005, p. 535) 32 Summary Table Of Gallbladder And Biliary System Procedures Procedure Anatomy Visualized Administration Of Contrast Media Cholecystography - Gallbladder Oral Cholecystogram (OCG) Gallbladder Oral ingestion Biliary ducts Direct injection through Cholangiography – Biliary Ducts Operative (immediate) cholangiogram / laparoscopic catheter during surgery cholangiogram T-tube cholangiogram Biliary ducts Direct injection through indwelling drainage tube Percutaneous Transhepatic Biliary ducts Cholangiogram (PTC) Direct injection by a needle puncture through the liver into the biliary ducts Endoscopic Retrograde Biliary / pancreatic ducts Direct injection through Cholangiopancreatogram catheter placed during (ERCP) endoscopic procedure Table 1-2 Summary Table Of Gallbladder And Biliary System Procedures (Bontrager & Lampignano 2005, p. 536) 33 34 RADIOGRAPHIC POSITIONING Oral Cholecystogram (OCG or Gallbladder) Routine 1. Posterior Anterior (PA) scout. 2. Left Anterior Oblique (LAO). 3. Right Lateral Decubitus. 4. Posterior Anterior (PA) erect. (Bontrager & Lampignano 2005, p. 537) Operative Cholangiogram Routine 1. Anterior Posterior (AP). 2. Right Posterior Oblique (RPO). (Bontrager & Lampignano 2005, p. 537) Percutaneous Transhepatic Cholangiogram (PTC) 1. Post-injection OP fluoro and spots. (Bontrager & Lampignano 2005, p. 537) T-Tube Postoperative Cholangiogram 1. Fluoro and spots films. 2. Anterior Posterior (AP). 3. Right Posterior Oblique (RPO). (Bontrager & Lampignano 2005, p. 537) Endoscopic Retrograde Cholangiopancreatogram (ERCP) 1. Post-injection AP fluoro and spots. 2. Anterior Posterior (AP). 3. Right Posterior Oblique (RPO). (Bontrager & Lampignano 2005, p. 537) 35 POSTEROANTERIOR (PA) PROJECTION : GALLBLADDER (ORAL CHOLECYSTOGRAM) SCOUT Pathology Demonstrated To adequate concentration of contrast media, correctness of exposure factors and to determine presence and location of gallbladder and choleliths, PA scout is taken. (Bontrager & Lampignano 2005, p. 537) Technical Factors Use image receptor (IR) size : 24 x 30 cm (10 x 12 inches) lengthwise or 35 x 43 cm (14 x 17 inches) lengthwise using moving or stationary grid. For the area of interest that have 16 cm thickness, the KvP range is 70-80 kVp and 22 mAs. (Bontrager & Lampignano 2005, p. 537) Shielding Lead shield is placed over gonadal area without obscuring area of interest. (Bontrager & Lampignano 2005, p. 537) Patient Position Patient is positioned in prone / erect position aided with pillow to support head. Patient’s arm up beside bed and legs extended with support under ankles. (Bontrager & Lampignano 2005, p. 537) 36 Fig. 2-5 Radiographic Positioning – Gallbladder (PA) (Chunggjaa 2010) Part Position Patient’s midsagittal plane is aligned to long axis of table with the right half of abdomen centered to central ray (CR) and to midline of table for sthenic body habitus type patient. Always make sure there is no rotation of pelvis or trunk. (Bontrager & Lampignano 2005, p. 537) Central Ray Central Ray (CR) is perpendicular to Image Receptor (IR). CR is at the level of L2 (1.25 to 2.5 cm above lowest margin of rib cage) and 5 cm to right of midsagittal plane for an average sthenic patient. Image receptor (IR) are centered to CR and the minimum source image distance (SID) is 40 inches (100 cm). (Bontrager & Lampignano 2005, p. 537) 37 Collimation The collimation are on four sides to cassette margins. (Bontrager & Lampignano 2005, p. 537) Respiration Patient’s respiration is suspended upon expiration. (Bontrager & Lampignano 2005, p. 537) Radiographic Criteria Structures Shown Center of the radiograph demonstrate the region of opacified gallbladder and area of cystic duct. (Bontrager & Lampignano 2005, p. 537) Position The lumbar vertebrae including the transverse processes appear symmetric as evident of no rotation exists. The spine also parallel to the edge of radiograph. (Bontrager & Lampignano 2005, p. 537) Collimation And CR On all 4 sides of image receptor (IR) are seen minimal collimation margins. CR is centered at level of gallbladder. (Bontrager & Lampignano 2005, p. 537) 38 Exposure Criteria Gallbladder or abdominal contents are project on radiograph with no motion artifact. Clearly visualize gallbladder even through overlying rib are the evident when appropriate technique is used. The choleliths also may be visible. (Bontrager & Lampignano 2005, p. 537) 39 LEFT ANTERIOR OBLIQUE (LPO) POSITION : GALLBLADDER (ORAL CHOLECYSTOGRAM) Pathology Demonstrated This positioning projects opacified gallbladder away from the vertebral column. It is also the ideal projection to delineate between gas trapped in bowel and radiolucent stones in the gallbladder. (Bontrager & Lampignano 2005, p. 538) Technical Factors Use image receptor (IR) size : 24 x 30 cm (10 x 12 inches) lengthwise using moving or stationary grid. For the area of interest that have 19 cm thickness, the KvP range is 70-80 kVp and 30 mAs. (Bontrager & Lampignano 2005, p. 538) Shielding Lead shield is placed over gonadal area without obscuring area of interest. (Bontrager & Lampignano 2005, p. 538) Patient Position Patient is positioned in semiprone position with left anterior side down aided with pillow to support patient’s head. Patient’s right arm up and the left one down. Patient’s right knee is partially flexed to maintain this position. (Bontrager & Lampignano 2005, p. 538) 40 Fig. 2-6 Left Anterior Oblique – Gallbladder (LAO) (Chunggjaa 2010) Part Position Patient is positioned into 15 ̊ to 40̊ left anterior oblique (LAO) (less rotation on broad hypersthenic and more rotation on thin asthenic type). Patient’s midsagittal plane is aligne to long axis of table, approximate right half of abdomen to central ray (CR) and to midline of table. An Right Posterior Oblique (RPO) projection may be perfomed if patient is not able to lie in a prone or semiprone position. (Bontrager & Lampignano 2005, p. 538) Central Ray Central Ray (CR) is perpendicular to Image Receptor (IR). CR is to gallbladder as determined from scout film. Image receptor (IR) are centered to CR and the minimum source image distance (SID) is 40 inches (100 cm). (Bontrager & Lampignano 2005, p. 538) 41 Collimation The collimation are on four sides to cassette margins. (Bontrager & Lampignano 2005, p. 538) Respiration Patient’s respiration is suspended upon expiration. (Bontrager & Lampignano 2005, p. 538) Radiographic Criteria Structure Shown Centered to IR are including entire opacified gallbladder and area of cystic duct. (Bontrager & Lampignano 2005, p. 538) Position The edge of radiograph is parallel to the spine. Gallbladder is adequately rotated away from spine. The patient is underoblique if the gallbladder is superimposed over any part of spine. (Bontrager & Lampignano 2005, p. 538) Collimation And CR On all 4 sides of image receptor (IR) are seen minimal collimation margins. CR is centered at level of gallbladder. (Bontrager & Lampignano 2005, p. 538) Exposure Criteria Gallbladder or abdominal contents are project on radiograph with no motion artifact. Clearly visualize gallbladder even through overlying rib are the evident when appropriate technique is used. (Bontrager & Lampignano 2005, p. 538) 42 RIGHT LATERAL DECUBITUS (PA PROJECTION) : GALLBLADDER (ORAL CHOLECYSTOGRAM) Pathology Demonstrated This positioning will project opacified gallbladder away from the vertebral column. It also will stratify any possible choleliths within the gallbladder. This positioning is an alternative way to perfomed biliary radiographic examination if patient cannot stand erect. (Bontrager & Lampignano 2005, p. 540) Technical Factors Use image receptor (IR) size : 24 x 30 cm (10 x 12 inches) lengthwise using moving or stationary grid. For the area of interest that have 17 cm thickness, the KvP range is 70-80 kVp and 26 mAs. (Bontrager & Lampignano 2005, p. 540) Shielding Lead shield is placed over gonadal area without obscuring area of interest. (Bontrager & Lampignano 2005, p. 540) Patient Position Patient is placed on separate radiolucent pad (for hips and shoulders to allow gallbladder to drop more freely away from the vertebrae) with the right side of the body is lying facing the table / IR. Pillow is provided for patient’s head with their arms are above their head and the knees flexed on on other. Secure cart wheels will make sure patient will not fall. Decubitus position provides for dropping of gallbladder away from spine wherein the stones are heavier than the bile layer out or separate from those lighter than bile. (Bontrager & Lampignano 2005, p. 540) 43 Fig. 2-7 Right Lateral Decubitus (PA) – Gallbladder (Chunggjaa 2010) Part Position Cart or IR are adjusted to center gallbladder to IR and to CR. Ensure hips and shoulders are in true lateral position with no rotation. (Bontrager & Lampignano 2005, p. 540) Central Ray Central Ray (CR) is horizontal to Image Receptor (IR). CR is directed to the right half of abdomen to gallbladder as determined from scout film. Image receptor (IR) are centered to CR and the minimum source image distance (SID) is 40 inches (100 cm). (Bontrager & Lampignano 2005, p. 540) Collimation The collimation are on four sides to cassette margins. (Bontrager & Lampignano 2005, p. 540) 44 Respiration Patient’s respiration is suspended upon expiration. (Bontrager & Lampignano 2005, p. 540) Radiographic Criteria Structure Shown Centered to IR are including entire opacified gallbladder and area of cystic duct. Gallbladder is seen located inferior vertebral column and stratification lines of choleliths should be visible if present. (Bontrager & Lampignano 2005, p. 540) Position The edge of radiograph is parallel to the spine. Gallbladder is adequately rotated away from spine. Bony lumbar spine structures are symmetric. (Bontrager & Lampignano 2005, p. 540) Collimation And CR On all 4 sides of image receptor (IR) are seen minimal collimation margins. CR is centered at level of gallbladder. (Bontrager & Lampignano 2005, p. 540) Exposure Criteria Gallbladder or abdominal contents are project on radiograph with no motion artifact. Clearly visualize gallbladder without overpenetrating and burning out possible choleliths are the evident when appropriate technique is used. (Bontrager & Lampignano 2005, p. 540) 45 POSTEROANTERIOR (PA) PROJECTION – ERECT POSITION : GALLBLADDER (ORAL CHOLECYSTOGRAM) Pathology Demonstrated This positioning will project opacified gallbladder away from the vertebral column. It also will stratify any possible choleliths within the gallbladder. (Bontrager & Lampignano 2005, p. 541) Technical Factors Use image receptor (IR) size : 24 x 30 cm (10 x 12 inches) lengthwise using moving or stationary grid. For the area of interest that have 17 cm thickness, the KvP range is 70-80 kVp and 30 mAs. (Bontrager & Lampignano 2005, p. 541) Shielding Lead shield is placed over gonadal area without obscuring area of interest. (Bontrager & Lampignano 2005, p. 541) Patient Position Patient is positioned erect, facing the table / IR with the arms at side. (Bontrager & Lampignano 2005, p. 541) Part Position Point on patient’s abdomen is align about 2 inches (5cm) to right of midsagittal plane to CR and to midline of erect table. Patient’s feet is spread to distribute body weight evenly on both legs for stabilization. Rotation into 10̊ to 15̊ LAO will shift gallbladder away from spine for asthenic type patient. (Bontrager & Lampignano 2005, p. 541) Central Ray Central Ray (CR) is horizontal and directed to gallbladder which will be 1 to 2 inches (2.5 to 5 cm) more inferior than on scout radiograph taken recumbent. Image receptor (IR) are centered to CR and the minimum source image distance (SID) is 40 inches (100 cm). (Bontrager & Lampignano 2005, p. 541) 46 Collimation The collimation are on four sides to cassette margins. (Bontrager & Lampignano 2005, p. 541) Respiration Patient’s respiration is suspended upon expiration. (Bontrager & Lampignano 2005, p. 541) Radiographic Criteria Structure Shown Centered to IR are including entire opacified gallbladder and area of cystic duct. Gallbladder is seen located at 1 to 2 inches (2.5 to 5 cm) more inferior than in recumbent position. Stratification lines of choleliths should be visible if present. (Bontrager & Lampignano 2005, p. 541) Position Spine is parallel to the edge of radiograph if there is no tilting in patient’s positioning. (Bontrager & Lampignano 2005, p. 541) Collimation And CR On all 4 sides of image receptor (IR) are seen minimal collimation margins. Gallbladder should not be superimposed by vertebra. (Bontrager & Lampignano 2005, p. 541) Exposure Criteria Gallbladder or abdominal contents are project on radiograph with no motion artifact. Clearly visualize gallbladder without overpenetrating and burning out possible choleliths are the evident when appropriate technique is used. No motion evident. (Bontrager & Lampignano 2005, p. 541) 47 48 CONCLUSION As a conclusion, there a several types of radiographic procedures in hepatobiliary system such as oral cholecystogram, percutaneous transhepatic cholangiogram (PTC), T-tube postoperative cholangiogram and endoscopic retrograde cholangiopancreatogram (ERCP). Besides the role of diagnostic procedure, one of the procedures which is endoscopic retrograde cholangiopancreatogram (ERCP) can also be the therapeutic procedure. As a radiographer, one should understand all the anatomy and physiology of the hepatobiliary system and master all the procedure associated to hepatobiliary system to make sure the diagnostic or therapeutic procedures of hepatobiliary system run smoothly and the patients will get the benefits from it. 49 REFFERENCES 1. Bontrager & Lampignano, S 2005, Textbook Of Radiographic Positioning And Related Anatomy, 6th edn. St. Louis, Missouri. 2. Ghimire, S.R. 2013, Hepatobiliary Apparatus : Gross Anatomy and Histology of the Liver and the Gallbladder. February 2013. Teaching Anatomy – Blogging Anatomy. Available from: <https://teachinganatomy.blogspot.com/2013/02/hepatobiliary-systemliver-and-gallbladder.html/>. [7 Disember 2013]. 3. Gallbladder body habitus, n.d. photograph. Available from: <http://www.duckskull.org/DMI%2063/1%20Biliary%20system/Pics%20for%20gi/gallb ladder%20body%20habitus.jpg/>. [2 Disember 2013]. 4. Meschan, I. 1955, An Atlas of Normal Radiographic Anatomy Saunders, London. Available from: < http://www.e-radiography.net/technique/chole/oral_chole.htm/>. [7 Disember 2013]. 5. Polaski & Tatro, 1996, T-tube placement in gallbladder surger. Available from: < http://medical-dictionary.thefreedictionary.com/gallbladder/>. [7 Disember 2013]. 6. Chapman & Nakielny, n.d. A guide to radiological procedures. Available from: < http://www.e-radiography.net/technique/ptc/ptc.htm/>. [2 Disember 2013]. 7. ERCP, n.d. Available from: < http://www.e-radiography.net/technique/ercp/ercp.htm/>. [2 Disember 2013]. 8. Cgunggja, V. 2010, Radiographic Positioning Playlist. Available from: < http://shelf3d.com/Search/Radiology%2BPositioning%2BPlayListIDPL37519A293DFD 1E9B?startIndex=30/>. [7 Disember 2013]. 50 DEPARTMENT OF MEDICAL IMAGING Assignment Submission Form Fill in the details: Name: Mohd Amir Syahmi Bin Mat Razali Student No: 2013226136 Part: HS242 / NHSIF5Y Course Name/Code: Specialized Radiographic Procedure / MRD551 Assignment Title: Investigation Of Hepatobiliary System Abnormalities Due Date: 9 Disember 2013 Submitted Date: 9 Disember 2013 Declaration “I hereby submit my assignment as part of fulfilling the requirement of the coursework assessment for (Course Name) Specialized Radiographic Procedure (Code) MRD551” Student Signature Date .......................................... 9 Disember 2013 _______________________________Tear Here__________________________________ CONFIRMATION OF ASSIGNMENT SUBMISSION To be filled by lecturer “I hereby confirmed the acceptance of the assignment for: (Course Name/Code): Specialized Radiographic Procedure” Lecturer Signature and Chop ................................................................... Date .............................. 51 52