Subspecialty Application Instructions and Eligibility
advertisement

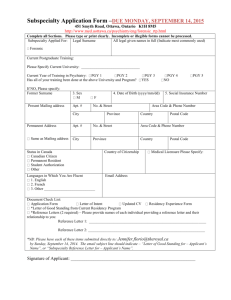
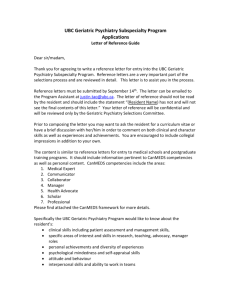
Subspecialty Application Instructions and Eligibility Applications for all 3 Subspecialty Programs for a July 2015 start are due Sunday, September 14, 2014. Eligibility: Child and Adolescent Psychiatry Subspecialty Program: All current PGY 4 or 5 residents are eligible to apply to the Child and Adolescent Psychiatry Subspecialty Program. Forensic Psychiatry Subspecialty Program: All current PGY 5 residents are eligible to apply to the Forensic Psychiatry Subspecialty Program. Geriatric Psychiatry Subspecialty Program: All current PGY 4 or 5 residents are eligible to apply to the Geriatric Psychiatry Subspecialty Program. For details about the programs, please refer to: http://www.psychiatry.utoronto.ca/education/subspecialties/ Those applicants who are selected for interviews will be notified October 1, 2014. Interviews will take place as follows: Child and Adolescent Psychiatry: October 20 -21, 2014 Forensic Psychiatry: October 21- 22, 2014 Geriatric Psychiatry: October 22, 2014 Submission Package: Applications MUST be submitted electronically to: cheryl.cawley@utoronto.ca All applications are to be completed by the submission deadline of Sunday, September 14, 2014: An application is deemed to be complete when all of the following components have been received: 1. Application Form: fully completed and signed 2. Updated CV 3. Letter of Intent 4. Residency Experience Form: fully completed 5. *Letter of Good Standing from Current Residency Program Director 6. *Reference Letters (2 are to be provided) *NB: Please have each of these items submitted directly to: cheryl.cawley@utoronto.ca by September 14, 2014. The email subject line should indicate – “Letter of Good Standing for – Applicant’s Name”, or “Subspecialty Reference Letter for – Applicant’s Name”. Any questions regarding the process can be directed to Cheryl Cawley either by telephone 416979-4699 or by e-mail: cheryl.cawley@utoronto.ca Subspecialty Application Form: DUE SUNDAY, SEPTEMBER 14, 2014 250 College Street, Room 840, Toronto, Ontario M5T 1R8 http://postgrad.utpsychiatry.ca/subspecialties/ Complete all Sections. Please type or print clearly. Incomplete or illegible forms cannot be processed. Subspecialty Applied For: Legal Surname All legal given names in full (Indicate most commonly used) Child & Adolescent Forensic Geriatric Current Postgraduate Training: Please Specify Current University: _______________________________ If NO, Please specify: Former Surname Present Mailing address 3. Sex Apt. # 4. Date of Birth (yyyy/mm/dd) No. & Street City Permanent Address Province 5. Social Insurance Number Area Code & Phone Number Country Postal Code Apt. # No. & Street Area Code & Phone Number City Province Country Postal Code address Status in Canada Country of Citizenship First Language Email Address 2. French Document Check List: Program – Please provide names of each individual providing a reference letter and their relationship to you: Reference Letter 1: ______________________________________________________________ Reference Letter 2: ______________________________________________________________ *NB: Please have each of these items submitted directly to: cheryl.cawley@utoronto.ca By: Sunday, September 14, 2014. The email subject line should indicate – “Letter of Good Standing for – Applicant’s Name”, or “Subspecialty Reference Letter for – Applicant’s Name”. Signature of Applicant: _______________________________________________________