Urinary Complaints/Positive Urine Culture
advertisement

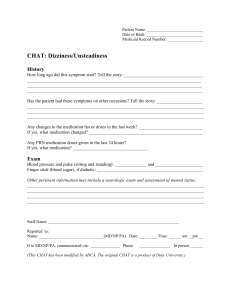
Patient Name: _________________________ Date of Birth: __________________________ Medicaid Record Number: ________________ CHAT: Urinary Complaints/Positive Urine Culture or UA History How long have the urinary symptoms been present? Tell the story: ______________________ ____________________________________________________________________________ ____________________________________________________________________________ ____________________________________________________________________________ Does the patient have a foley catheter? ______________________________________________ Has the patient been on antibiotics this week? ________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ Current symptoms or complaints: □ pain with urination □ urinary frequency □ blood in urine □ foul-smelling urine □ inability to urinate or difficulty passing urine □ urinary incontinence □ decreased amount of urine Exam Temperature, blood pressure, pulse _________________________________________________ Staff Name: _______________________________________________________(RN/LPN) __________ Reported to: Name: _______________________________ (MD/NP/PA) Date: _________ Time: _____am __ pm __ If to MD/NP/PA, communicated via: ______________ Phone _______________ In person ______ (This CHAT has been modified by AHCA. The original CHAT is a product of Duke University.) Patient Name: ___________________________ Date of Birth: ___________________________ Medicaid Record Number: _________________ CHAT Progress Note Progress Note (complete and place CHAT/progress note in medical record) _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ __ Family or health care proxy notified Return call/new orders from MD/NP/PA Date___/___/___ Time___/___AM/PM Signature________________________________RN/LPN Date___/___/___ Time___/___AM/PM (This CHAT has been modified by AHCA. The original CHAT is a product of Duke University)