Efficiency of Enterosgel in kidney diseases in children
advertisement

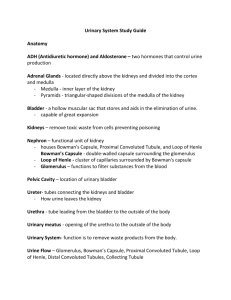
Efficiency of Enterosgel in kidney diseases in children living in the the cement industry region. Kudin M.V., Tsaregorodtsev A.D., Fedorov Y.N., Dlin V.V. Federal State Budget Institution "Moscow Scientific and Research Institute of Pediatrics and Pediatric Surgery", Russian Ministry of Health Nowadays the problem of interaction between the environment chemical composition and the health of the population is a challenge not only in Russia but also in other parts of the world [1, 2]. The level of overall health and quality of the environment (taking into account natural and anthropogenic factors) are to different extent determined by biogeochemical features in different regions of Russia. With intensification of industrial and human activities, urban growth, creation of "megalopolises" and major industrial centers the load has increased so intensively that a special ecological environment was formed, with high concentrations of anthropogenic products – i.e. with a serious pollution of air, soil and water basins [3]. The contribution of anthropogenic environmental risk factors in the incidence of diseases in children and adolescents, is 10-60% according to WHO. In the recent decades, study of diseases caused by ecological factors related to toxic effects of the environment primarily of anthropogenic origin is being developed. Among them, the increasing attention is drawn to kidney diseases caused by exposure to heavy metals, especially in childhood. Thus, kidney diseases caused by ecological factors in childhood often lead to the development of progressive diseases in adults [4, 5]. One of pollution sources of the biosphere is chemical industry, including cement production. According to regulations on quality control and environmental safety by international standards, cement production is a source of mercury, strontium and zinc accumulation in the soil. The main impact on the environment in cement production is associated with emissions of quickly evaporating components in the form of dust, which in most enterprises exceeds the values allowable for Russian national requirements [6, 7]. As a result of water and air transport of these toxicants, areas located at a considerable distance may become contaminated. Analysis of epidemiological data suggests that occupational diseases due to contact with the cement during the production are among the most common [8, 9]. Data on the incidence in the population of an area with cement industry are insufficient. According to research of Dlin V.V. et al. (1994) [10], in the areas around a large cement plant "Bryanskcement" the frequency of renal pathology in children was significantly higher than the average Russian figure (29:1000) and was as high as 266 per 1,000 children examined. In the structure of renal disease patients with predominated urinary tract infection (40%) and dysmetabolic nephropathy (11%) dominated, while phosphate-calcium crystalluria was detected more frequently than calcium-oxalate (50% and 15%, respectively), membranopatologic disorders were detected as well. According to Saratov special inspection of environmental control, pollution by chemical elements including salts of heavy metals, in Volsk, Saratov region was: chrome – 1.5-8.6 times greater than the maximum permissible concentration (MPC), zinc - 1.5-1.9 MPC, copper - 2-7 MPC, nickel 1,2-7 MPC, cadmium 2.3-16 MPC, lead 2.6 MPC, cobalt - 1.5-2.3 MPC [11]. High frequency of kidney diseases in children living in adverse environmental conditions result in the the need to find treatment and prevention methods. In this respect, use of enterosorbent Enterosgel seems interesting, which has shown the high clinical efficiency in the treatment of dysmetabolic nephropathy [Gordeeva E.A., Alekseeva N.V., Kon’ I.J. et al, Use of enterosorbent Enterosgel in children with dysmetabolic nephropathy / Pediatrics, No. 4 - 2005 - P.79-82]. Furthermore, enterosorbent has been successfully used to remove heavy metals and radionuclides from the body. Thus, it has been proved that Enterosgel helps to normalize the function of the excretory system by reducing the load on the natural detoxification system, in particular by increasing the ability of serum proteins to bind toxins [Osadchaya O.I., Boyarskaya A.M. Clinical efficacy of enterosorption for relief of endogenous intoxication in patients with chronic ulcerative colitis/ Liki Ukraini, No. 6 (132). - 2009. - P. 87-89.] Objectives: To determine the effectiveness of enterosorbent Enterosgel in kidney diseases of children living in the areas of cement industry. Characteristics of the surveyed groups of children and methods A three-stage nephrology survey included 5851 children (M / W 2904/2947; 3,316 children aged 1 to 6 years and 2,535 children - from 7 to 18 years) living in the city of Volsk - a major center of the cement industry (the main region). A similar program included 630 children (M / W 283/347; 158 children - 1-6 years, 472 children - 7-18 years) from the control region (village Cherkasskoye), located at a distance of 50 km. a screening was conducted at Stage 1 (Table 1); at Stage 2 - in-depth examination including urinalysis, urine culture for flora, daily proteinuria and ultrasound examination of the urinary system; at Stage 3 children who had any changes at Stage 2 were examined in the local or regional nephrology departments with conduction, if necessary, of urorentgenology surveys and urine quantitative studies. Laboratory and instrumental studies included in the three-stage examination are presented in Table 1. Table 1. Lab tests used within the three-stage examination No . Studied values Number of children Study methods Stage 1 1. Studies of urobilinogen, glucose, bilirubin, ketones (acetoacetic acid), specific gravity, occult blood, рН, protein, nitrites, leukocytes and ascorbic acid in the urine Main group – 5851 Express-analysis (in vitro) with reactant strips CYBOW (Korea, South) и DEKA PHAN Control group LEUCO (Czech Republic) – 630 Stage 2 2. Urine RBC and WBC, miscroscopy for chtystalluria urine Main group – 4147. Control group – 304 Nechiporenko test, first void urine miscroscopy 3. Size of kidneys, parenchyma, state of pelvicalyceal system, vesicoureteral reflux, bladder state. Main group – 4147. Control group – 304 Ultrasound study of kidneys and urinoexcretory system (apparatus MyLab-15, Netherlands, with convex realtime linear transducer). 4. Urine protein (24 h) Main group – 4147. Control group – 304 With nitric acid (Roberts method) 5. Definition of bacteriuria (for the main indication) Main group – 911. Control group – 112 Method of urine culture on Petri dish with nutrient agar (Endo or Mc Conkey agar) Stage 3 6. Hb, erythrocytes, blood sedimentation rate, leukocytes and blood fromula Main group – 1706. Control group – 110 CBC 7. Serum protein, proteinogram, холестерин, β-lipoproteins, urea, creatinin, antistreptococcus antibodies titres Main group – 1706. Control group – 110 Standard methods of biochemical blood count 8. Size of kidneys, parenchyma, state of pelvicalyceal system, vesicoureteral reflux, bladder state. Main group – 1706. Control group – 110 Ultrasound of kidneys and urinoexcretory system, for the main indication: intravenous urography, voiding cystography 9. Creatinine concentration in the blood serum, glomerular filtration rate (Schwarz formula), water reabsorption rate 10. Definition oft he distal tubule function: - study of concentration function; Main group – 1706. Control group – 110 Jaffe reaction on the photoelectric calorimeter, Main group – 1706. Control group – 110 Zimnitsky test, blood and urine osmolarity by electrothermal method, on the osmometer ОМКА 1ц – 01 Reberg test - acidogenic function of kidneys Urine рН (test strips), evaluation of ammonia in the study of uroproteinogram and aminoaciduria 11. - oxalate excretion Sivorinovsky method (1969) Of the children identified at Stage 3, 31 children with nephropathy (main group) from the core region were selected for further treatment with Enterosgel (M / W 14/17; mean age 9.65 ± 1.13 years). Enterosgel was administered at a dose 1 dessert spoon 3 times a day, daily dose - 30 g for 1 month without concomitant therapy, including antibiotic therapy. The control group consisted of 30 children with nephropathy from the same region, who did not receive Enterosgel (M / W 16/14; mean age 7.59 ± 1.29 years). The main group included 17 (54.8%) of children with urinary system infection (USI), and 14 (45.2%) - with dysmetabolic nephropathy; the control group - 19 (63.3%) children with USI and 11 (36.7%) - with dysmetabolic nephropathy. The groups did not differ significantly by gender, age and clinical diagnosis. Clinical and laboratory examination and quantitative study of the chemical composition of biological media (urine, nails, hair) was performed over time before treatment and 2 weeks after the end of treatment in children of the main group and after 6 weeks of observation in children of the control group. The reference content of chemical elements in the urine was considered that of urinary excretion in healthy children from potentially clean regions. Studies of chemical composition of biological media over time in children of the main group, the control group and in healthy children from potentially clean regions were conducted in the test analysis center (head of the center - MD, Professor Yakshin V.V.), State Unitary Enterprise "Russian Research Institute of Chemical Technology ", Russian Ministry of Atomic Energy by atomic absorption spectrophotometry with inductively-coupled plasma ionization, on the apparatus «Varian Vista Pro CCD Simultaneous ICP-OES »(USA) Results High rates of renal disease resulting from the three-stage nephrological examination was a confirmation of the impact of ecopathogens on renal tissue of children living in the area of cement production. Figure 1 shows the overall prevalence rates of renal diseases and certain clinical forms in comparison with potentially safe (control) region. 174,6 Распространенность нефропатий: 291,6 хронический обструктивный… тубулоинтерстициальн ый нефрит инфекция мочевой системы 15.9 28,2 0 1,9 34.9 49.2 139.7 дисметаболическая нефропатия 240.5 0 Группа сравнения 100 200 300 Основная группа Figure 1. Incidence of renal diseases according their nosology in children of the main and control region (per 1000 examined children) Figure captions: /Incidence of nephropathy – chronic obstructive kidney disease – tubular interstitial nephritis – urinary system infection – dysmetabolic nephropathy/ Main group – Control group/ The effectiveness of treatment was assessed in terms of urinary syndrome dynamics, urine oxalates and urinary excretion of chemical trace elements of danger classes 1 and 2 in children before and 2 weeks after the end of the four-week course of treatment, i.e. 6 weeks after the first examination. Table 2 shows the dynamics of indicators of bladder syndrome and quantitative content of urine oxalate in children treated with Enterosgel and in the control group at 6 weeks after the initial examination. Table 2. Dynamics of urinary syndrome and quantitative indicators of oxalates No. Value Main group (Enterosgel) n=31 Control group n=30 1. 2. Protein, mg/l WBC, µl 3. RBC, µl 4. Oxalates, mg/24 h 2 weeks after end of treatment 33,0±5,8 15,7±2,8 34,95± 47,52±15,21 13,12 р Initial After6 weeks р <0,05 29,00±5,4 48,71± 21,02 14,00± 11,17 31,0±5,8 45,24± 10,69 10,09± 9,11 57,92± 2,75 >0,05 Initial >0,05 14,33±11,12 4,21± 2,15 <0,05 64,09±3,56 39,18± 4,23 >0,05 64,68± 3,26 >0,05 >0,05 >0,05 In the group of children with renal disease treated with Enterosgel proteinuria decreased more than twice, leukocyturia – by 1.43 times, erythrocyturia – by 3.4 times, oxaluria – by 1.6 times. In the control group no significant differences were found in the content of oxalates and bladder syndrome: a protein, leukocytes, erythrocytes, Table 3 Dynamics of urinary syndrome and oxaluria on the background treatment, with the nosology No. 1. 2. Gorup Protein WBC RBC Oxalates % % % % Decrease 93,5 45,2 77,4 48,4 No changes 6,5 41,9 16,1 32,3 Increase Including urinary Decrease system infection No changes (n=17) Increase 0 94,1 5,9 0 12,9 29,4 47,1 23,5 6,5 94,1 5,9 0 19,3 52,9 35,3 11,8 With dysmetabolic nephropathy (n=14) Decrease No changes Increase 92,9 7,1 0 64,3 35,7 0 57,1 28,6 14,3 42,8 28,6 28,6 Control group n=30 Decrease 13,3 33,3 30,0 30,0 No changes 60,0 53,4 56,7 60,0 Increase Including urinary Decrease system infection No changes (n=19) Increase With Decrease dysmetabolic No changes nephropathy Increase (n=11) 26,7 5,3 57,9 36,8 27,3 63,6 9,1 13,3 31,6 52,6 15,8 36,4 54,5 9,1 13,3 36,8 52,6 10,5 18,2 63,6 18,2 10,0 42,1 57,9 5,2 18,2 63,6 18,2 Main group (Enterosgel) n=31 Value dynamics In the study group, in most children proteinuria and microhematuria decreased, and in almost half of the cases – leukocyturia and oxaluria. Increase of values was marked only in few cases. Similar results were observed in the group of children with urinary infection and with dysmetabolic nephropathy, except less frequent reduction of microhematuria in children with dysmetabolic nephropathy (p <0.05) (Table. 3). In contrast, positive dynamics in the comparison group was noted in less than a third of cases and did not differ depending on nosology. Thus, in the main group of children with renal disease in the region of cement production improvement of urine values was demonstrated two weeks after the end of treatment with Enterosgel in most cases, while without therapy with Enterosgel, either urinary symptoms or oxaluria severity were maintained or the increase was observed. Moreover, in all groups of children before and 2 weeks after the end of the 4-week course of treatment, i.e. 6 weeks after initiation of therapy following trace elements were studied in the urine over time, depending on the hazard class. Hazard class 1: cadmium (Cd), arsenic (As); hazard class 2: antimony (Sb), chromium (Cr). Table 4 shows the contents of chemical elements in the urine of children before and after treatment with enterosorbent Enterosgel and in the comparison group. During treatment with Enterosgel showed a significant increase in urinary excretion of toxic trace elements in children: cadmium 2.2 times (p <0.05), antimony 2.7 times (p <0.05), arsenic - 1.75 times and Cr - 1.3 times in contrast to the comparison group, where the essential dynamics were observed. Table 4 Dynamics of excretion of chemical elements (mg/l) in the urine of children treated with Enterosgel Control groups, n-30 Main group, n-31 N o. Chemical elements Initial Two weeks after the 4week treatment р Initial After 6 weeks р 1 Cadmium (Cd) 0,025±0,00 4 0,06±0,003 <0,0 5 0,001±0,000 0,001±0,000 >0,05 1 1 2 Arsenic (As) 0,004±0,00 1 0,007±0,001 >0,0 5 0,005±0,000 0,007±0,002 >0,05 1 3 Antimony (Sb) 0,015±0,00 1 0,04±0,001 <0,0 5 0,011±0,002 0,012±0,001 >0,05 4 Chrome (Cr) 0,09±0,001 0,12±0,02 >0,0 5 0,12±0,05 0,13±0,05 >0,05 Conclusion It has been established that the incidence of renal diseases in children in the regions of cement industry is very high, especially regarding dysmetabolic nephropathy, unlike the control region, which shows the significant role of environmental factors in the development of renal damage. The conducted studies of Kudin M.V. (2012) [12] have shown that in children and adults living in the area and having no renal diseases cadmium - toxic element, hazard class 1 - accumulates in kidney tissue, which justifies the use of enterosorbent Enterosgel in persons living in the region as a prophylactic purpose. Enterosgel not only prevents accumulation of toxic substances into the body by their intestinal adsorption, but also contributes to the removal of heavy metals from the urinary system. Inclusion of Enterosgel in the therapy of children with renal diseases living in the region of cement industry leads to the increased urinary excretion of cadmium, chromium, antimony, and arsenic and improvement of urinary symptoms and, above all, reduction of proteinuria, reflecting improved reabsorption function of the epithelium of proximal tubules. No undesirable effects have been registered in children receiving Enterosgel. References 1. Saet Y.E., Revich B.A., Yanin E.P. et al. Geochemistry of the environment. - Moscow: Nedra, 1990. – 335 p. 2. Negretti de Bratter V. Epidemiological occurrence of trace element deficiency in childhood and treatment concept. // TOPIC-10. Evian. May 3-7, 1999. - Evian, 1999. - P.75. 3. Veltishchev Y.E., Fokeeva V.V. Environment and children's health. Chemical Ecopathology. Lecture / Application, Russian bulletin of perinatology and pediatry - Moscow, 1996. - 60 p. 4. Ignatov M.S., Harina E.L., Dlin V.V. et al. Role of heavy metals in the genesis and progression of pathology of urinary system organs. / Thesis of 1st Nephrology Congress of Russia. - Kazan. 1994. - P.18-19. 5. Osmanov I.M. Clinico-pathogenic features and tactics of treatment of renal lesions in children in ecologically unfavorable regions. // Thesis abstract for MD dissertation. - Moscow. - 1996. – 46 p. 6. Revich B.A. Scientific bases of hygiene research of city environment using geochemical methods. // Thesis abstract for MD dissertation. - Moscow. - 1992. – 48 p. 7. Kudzin M.M. Recording and analysis of environmental costs in cement production. Thesis abstract for MD dissertation - Saratov, 2010. - 18 p. 8. Retnev V.M., Ivanov F.A., Petrunya Y.A. On the prevalence of pneumoconiosis in cement plants (review). // Occupational Medicine and Industrial Ecology. - 2002. - 1 - P. 26-31. 9. Dickel H., Kuss O., Schmidt T.L. Occupational relevance of positive standard patch-test results in employed persons with an initial report of an occupational skin disease. // Int. Arch. Occup. Environ. Health. - 2002. - 75 (6). - R.3-34. 10. Dlin V.V., Ignatov M.S., Kaganov S.Y. et al. Medical and environmental health assessment of the child population in the area of cement production. // Scientific and practical conference "Ecology of childhood: social and health problems." – St. Petersburg. - 1994. - P.69-71. 11. On the state of the environment of Saratov region in 2009 / Report. - Saratov, 2009. – 180 p. 12. Kudin M. Laws of pathological processes of the urinary system in children living in the area of cement production, and treatment optimization. // MD dissertation. - Moscow. - 2012. – 581 p.