Dizziness, Unsteadiness

CHAT: Dizziness/Unsteadiness
Patient Name: ___________________________
Date of Birth: ___________________________
Medicaid Record Number: _________________
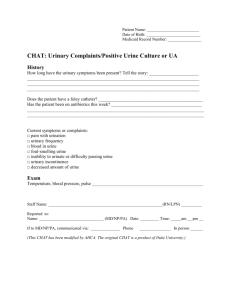
History
How long ago did this symptom start? Tell the story: ___________________________________
_____________________________________________________________________________
_____________________________________________________________________________
_____________________________________________________________________________
Has the patient had these symptoms on other occasions? Tell the story: ____________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Any changes to the medication list or doses in the last week? ____________________________
If yes, what medication changed? __________________________________________________
Any PRN medication doses given in the last 24 hours?
If yes, what medication? _________________________________
Exam
Blood pressure and pulse (sitting and standing): ______________ and _____________________
Finger stick (blood sugar), if diabetic: _______________________________________________
Other pertinent information may include a neurologic exam and assessment of mental status .
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Staff Name: _______________________________________________________________
Reported to:
Name: _______________________________(MD/NP/PA) Date: _________Time: ______ am __pm __
If to MD/NP/PA, communicated via: ______________ Phone _______________ In person ______
(This CHAT has been modified by AHCA. The original CHAT is a product of Duke University.)
Patient Name: ___________________________
Date of Birth: ___________________________
Medicaid Record Number: _________________
CHAT Progress Note
Progress Note
(complete and place CHAT/progress note in medical record)
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
__ Family or health care proxy notified
Return call/new orders from MD/NP/PA Date___/___/___ Time___/___AM/PM
Signature________________________________RN/LPN Date___/___/___ Time___/___AM/PM
(This CHAT has been modified by AHCA. The original CHAT is a product of Duke University)