Spontaneous Urticaria and Angioedema
advertisement

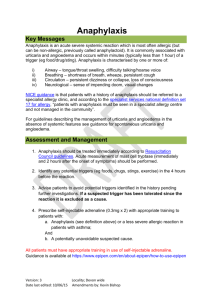
Spontaneous Urticaria and/or Angioedema Key Messages Urticaria and angioedema may be allergic or non-allergic (spontaneous). In spontaneous urticaria/angioedema there may be exacerbating factors (eg heat, cold, pressure, stress, some medications). Acute urticaria (lasting less than 1-2 days) do not need routine referral unless there are specific questions. This referral pathway deals with chronic urticaria only. Assessment The clinical history of the symptoms and suspected precipitants/exacerbating factors is paramount, along with examination of the symptoms if possible. The history should include - Date of onset - Nature and severity of symptoms - Exacerbating factors (eg heat, cold, pressure, stress, medications) - Treatment required and efficacy - Thorough assessment to exclude underlying pathology (eg chronic infection) - Suspected triggers (likely only if the symptoms are predictably associated with exposure, and remit upon avoidance. If the symptoms persist despite avoidance the suspect can be excluded as a cause). - If associated with airway/breathing/circulation/neurological features see anaphylaxis pathway - If history suggests food or drug allergy (in the absence of anaphylaxis) please click for appropriate pathway. ACE inhibitor treatment can cause angioedema (without urticaria) even after months or years of treatment and must be stopped in patients presenting with angioedema. Angioedema in the absence of urticaria also raises the possibility of hereditary/acquired angioedema; check complement C4 to exclude this. Investigations No investigations are routinely indicated, and should only be performed if there is a specific indication. The exception is complement C4 levels in angioedema alone. Management 1. Spontaneous urticaria and angioedema should be treated initially with nonsedating antihistamines. Version: 3 Date last edited 10/06/15 Locality: Devon wide Amendments by: Kevin Bishop a. Treatment may be as required or prophylactic depending on symptom frequency of symptoms. b. Higher than licensed doses may be required (eg cetirizine 10mg or fexofenadine 180mg up to 4x/day). This is supported by British and European guidelines and there is good safety data. c. These increased doses must not be used in pregnancy, and attention should be paid to interactions with other drugs. 2. Swelling involving the mouth/tongue can cause patients considerable concern. If tongue swelling is mild treatment with additional antihistamine and a single dose of prednisolone 20-30mg may be used. a. Long term regular corticosteroids are not advised. 3. Any systemic involvement (eg airway, breathing, circulation, neurological) prescription of 2 x 0.3mg self-injectable adrenaline pens, instruction in their use, and be referred to a specialist allergy service. 4. All patients with angioedema should avoid ACE inhibitors. 5. Patients with urticaria and/or angioedema should be advised to use NSAIDS with caution. Referral Referral criteria 1. Patients with troublesome symptoms (rash or swelling) despite high dose prophylaxis with non-sedating antihistamines (3-4x/day). a. Ranitidine 150mg BD +/- montelukast 10mg daily may be tried in addition to antihistamines. 2. Any systemic features to suggest anaphylaxis. 3. If there is diagnostic uncertainty 4. Patients with angioedema and a low C4 Referral Instructions Refer to Peninsula Immunology and Allergy Service Refer via DRSS for NEW Devon CCG patients Choose and Book Selection Specialty: Allergy Clinic type: Allergy Service: DRSS- Western –Allergy & Immunology - CCG - 99p Referral forms DRSS Referral form Version: 3 Date last edited 10/06/15 Locality: Devon wide Amendments by: Kevin Bishop Supporting Information http://www.guidelines.co.uk/skin_bsaci_urticaria_angio http://onlinelibrary.wiley.com/doi/10.1111/cea.12494/pdf http://southwest.devonformularyguidance.nhs.uk/formulary/chapters/3.respiratory/3.4.1-antihistamines www.ga2len.net/464D9d01.pdf Patient Information http://www.patient.co.uk/health/chronic-urticaria-hives Pathway Group This guideline has been signed off by the Western Locality on behalf of NEW Devon CCG. Publication date: June 2015 Review date: May 2017 Version: 3 Date last edited 10/06/15 Locality: Devon wide Amendments by: Kevin Bishop