Food Reactions - Plymouth Hospitals
advertisement

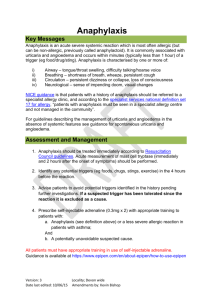
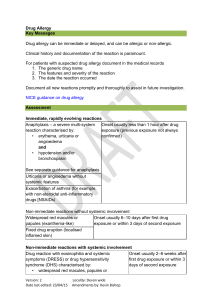
Food Allergy Key Messages Anaphylaxis is an acute severe systemic reaction which is most often allergic (but can be non-allergic, previously called anaphylactoid). It is commonly associated with urticaria and angioedema and occurs within minutes (typically less than 1 hour) of a trigger (eg food/drug/sting). Anaphylaxis is characterised by one or more of: i) ii) iii) iv) Airway – tongue/throat swelling, difficulty talking/hoarse voice Breathing – shortness of breath, wheeze, persistent cough Circulation – persistent dizziness or collapse, loss of consciousness Neurological – sense of impending doom, visual changes Less severe reactions are common, and warrant avoidance of the food in all cases and further investigation in certain circumstances. Assessment Type 1 hypersensitivity reactions to food are usually (but always) associated with one or more of urticaria, angioedema, or local oral symptoms, and occur within minutes (typically less than 1 hour) of ingestion. If there are associated systemic features refer to anaphylaxis guidance. The symptoms of non-type 1 hypersensitivity (food intolerance) are often gastrointestinal only, and the timing is often not suggestive of type 1 hypersensitivity. Eczema alone is not caused by food allergy in adults and this should not be a focus of investigation. Clinical history and documentation of reactions is paramount. Document all new reactions promptly and thoroughly to assist in future investigation. Include: - Foods and medications consumed within 4 hours prior to the reaction - Activities/exercise/exposures over that period - Tolerance of these foods/drugs since the episode (this excludes these as a cause of the reaction). - Any dietary implications (eg nut allergy in a vegetarian or coeliac disease patient). - Any other foods that are avoided and the reason for avoidance Investigations If a food is clearly implicated request specific IgE to the particular food. There is no role for measurement of total IgE, and do not request testing against foods which were not involved, or which have been tolerated since the reaction. Version: 2 Date last amended: 23/04/15 Locality: Devon wide Amendments by: Kevin Bishop Patch testing, skin prick testing, and oral food challenges should not be undertaken in primary care. Management 1. Anaphylaxis should be treated immediately according to Resuscitation Council guidelines. Acute measurement of mast cell tryptase (immediately and 2 hours after the onset of symptoms) should be performed. 1. Advise patients to avoid potential triggers identified in the history pending further investigations. If a suspected trigger has been tolerated since the reaction it is excluded as a cause. Advise particular caution when eating away from home or with food not prepared by the patient. 2. Negative specific IgE does not completely exclude food allergy or intolerance a. If there is strong clinical suspicion referral to a specialist allergy clinic should be considered. 3. All patients should be provided with an emergency plan. a. Self-injectable adrenaline should be prescribed i. Where there were features of anaphylaxis (airway, breathing, circulation, or neurological), ii. For all patients with food allergy and a history of asthma iii. For patients where access to emergency services might be delayed (eg living in a rural location, travelling to remote area with limited access to healthcare) b. Patients with self-injectable adrenaline must have appropriate training. Guidance is available at https://www.epipen.com/en/about-epipen/howto-use-epipen 4. The use of unorthodox methods of diagnosis (eg naturopathy, food-specific IgG testing, vega testing, kinesiology, pulse testing, hair analysis) or treatment (eg homeopathy, acupuncture, reflexology, chiropractic therapy, or osteopathy) has no evidence and should not be used. Referral Referral Criteria 1. All patients with anaphylaxis unless there is a simple trigger and no cofactors (eg asthma, cardiovascular disease). 2. Patients with suspected food reactions where food trigger is not clear (eg negative specific IgE testing to the suspected food). Version: 2 Date last amended: 23/04/15 Locality: Devon wide Amendments by: Kevin Bishop 3. Where multiple foods are implicated 4. Where avoidance would cause important dietary restriction (eg nuts in a vegetarian or coeliac disease patient) 5. Where the allergy has occupational implications (eg military employment). Referral Instructions Referral Instructions Refer to Peninsula Immunology and Allergy Service Refer via DRSS for NEW Devon CCG patients Choose and Book Selection Specialty: Allergy Clinic type: Allergy Service: DRSS- Western –Allergy & Immunology - CCG - 99p Referral forms DRSS Referral form Supporting Information This guideline has been signed off by the Western Locality on behalf of NEW Devon CCG. Publication date: June 2015 Review date: May 2017 Version: 2 Date last amended: 23/04/15 Locality: Devon wide Amendments by: Kevin Bishop