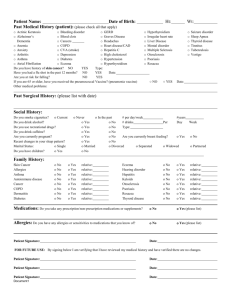
Initial Assessment Form
advertisement

Occupation (if any):________________________________ Place sticker here. What is the reason your doctor sent you to see us? . ________________________________________________ How long have you had this problem? _________________ How much of a problem is this condition for you? O Not at all O A little O Somewhat O Quite a lot O Extremely What treatments have you used for this problem? ________________________________________________ Do you have any other medical problems? _____________________________________________________ What are your current medications?___________________________________________________________ Do you have any drug allergies? _____________________________________________________________ Do you have a family history of medical /skin problems?__________________________________________ Do you have a medication plan? (i.e. Green Shield):______________________________________________ Are you interested in clinical research trials regarding your condition? Yes □ No □ Section below for office use only--------------------------------------------------------------------------------Management: Diagnosis: ______________________________________ ______________________________________ ______________________________________ Return visit: ____________ A/E’s: ____________________________ SPF _______ Info Pamphlet: Acne / Eczema / Psoriasis Rosacea / Moles / Urticaria Pre-op: __allergy to numbing __artificial joints __blood thinners __heart murmur/valves __fainting tendency __pacemaker