cmc rotation dates: ______ school
advertisement

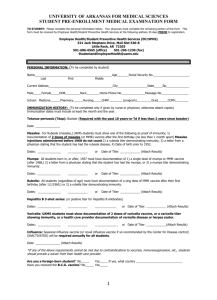
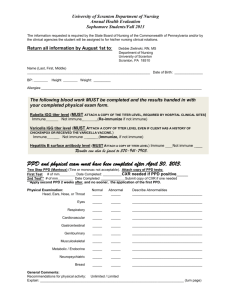
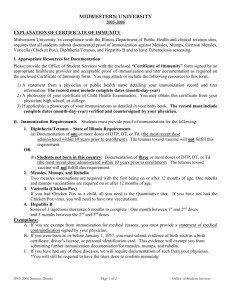
REQUIRED INFORMATION FORM- FOR FACULTY, STUDENTS & CONTRACT STAFF NAME: ___________________________ HOME PHONE: _______________________ CMC ROTATION DATES: ___________ SCHOOL: _____________________________ ADDRESS: ________________________ CITY: ________________________________ FACULTY: ________________________ SCHOOL PHONE: ______________________ Please provide the following information – submit at least 1 week before the start of clinical rotation. 1. You must have a negative TB test (TST) within the last 12 months prior to your clinical rotation. If you have had a positive TB test, you must have a negative chest x-ray within the last 5 years. If positive, include mm (millimeters) of induration ________ mm. TB Test: Date: ________ Positive ______mm induration (if TB skin test) Negative ______ Chest X-Ray: Date: ________ Positive _______ Negative ______ (please attach x-ray report) 2. Date of birth:__________________ Have you had the chickenpox (Varicella)? _____ yes ______no. If NO or if you were born in or after 1980, you must have two doses of Varivax vaccine or a positive titer: Dose #1_________ Dose #2_________ Varicella titer date____________result__________________ 3. EVERYONE must demonstrate immunity to measles, mumps, and rubella. A. Were you born prior to January 1, 1957? If YES: have you had the Measles (Rubeola)? have you had the Mumps? ____yes ____no. ____yes ____no. ____yes ____no. ******If no history of disease, date of MMR vaccine _________****** Must have rubella vaccination or positive titer – vaccine date_______ titer date/result____________ B. If NO: (born after 1-1-1957) Must have 2 MMR vaccinations or positive titers to all three Measles vaccine or titer date ______ titer result _______ Rubella vaccine or titer date______ titer result _______ Mumps vaccine or titer date______ titer result _______ OR _ MMR #1 _________ date MMR#2 __________ date You must have 2 doses of measles (rubeola) vaccine, 2 doses of mumps vaccine and 1 dose of rubella vaccine or 2 MMR’s or have evidence of immune titers for all three 4. Have you had the Hepatitis B Vaccine? _______ Date of last dose ____________Dose # _______ 5. Date of CPR expiration _____________ Course Type _________________ 6. Have you viewed the Children’s Annual Training Video (CART) and completed the post-test? _____yes _______no 7. Record of a Td (Tetanus/Diphtheria) or Tdap (Tetanus/Diphtheria/Pertussis) within the past ten years. If in direct patient care, must have received one dose of Tdap vaccine. Date_________ Td / Tdap (please circle). 8. Influenza vaccination (required annually) Revised 09-20-11 C Amrich if yes, how many doses have you received? ____________ Vaccine immune titer date & results _________________ Date___________________________