Brigham and Women`s Hospital & Faulkner Hospital
advertisement

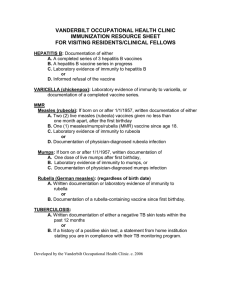
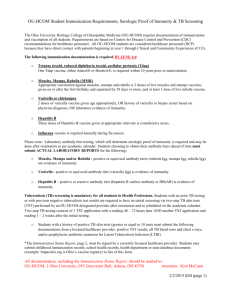
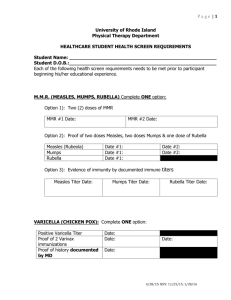
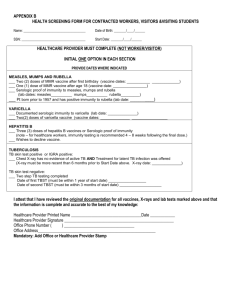
Partners HealthCare System, Inc. Temporary Staffing - Background Check Requirements Completion Certification Form [VENDOR LEGAL NAME] attests that the following items below have been verified for this employee: Vendor’s Employee Name: Residential Address: Telephone Number: Position: Position Location: Drivers License Number: Vendor must fill in and sign the completed form then e-mail to MGH/Security prior to the listed individual’s project start date. Please email to: policecori@partners.org For returning vendor employees - background checks cannot be older than six months. If a vendor employee is working for a program regulated by an agency i.e. EOHHS, DPH, Children's Services etc the CORI may be more frequent BACKGROUND INFORMATION Description Social Security Number Trace Shows where an individual lived, worked and/or went to school for the past 7 years Comments: Criminal Background Screen Multi-state criminal background check by counties lived, worked and/or attended school for past 7 years. Any record(s) to be vetted with MGH/Security for a final decision: policecori@partners.org Comments: Exclusion Check Search OIG and GSA databases (process equivalent to Partners CBI checks of employees). Potential matches to be vetted by Corporate Compliance for a final decision: PHSComplianceExclusion@partners.org Comments: CORI "proper" Provides criminal history for the state of Massachusetts going back to age 17. Any record(s) to be vetted with MGH/Security for a final decision: policecori@partners.org Comments: 1 Verified Partners HealthCare System, Inc. Education Highest level education achieved (HS/AS/BA/MA/advanced degree and/or certification if required for the position). If not able to verify stated education then the individual is not eligible to be placed at Partners HealthCare Comments: Professional Licenses/Certification Have a current professional license and/or certification, if required for the position Comments: INFECTION CONTROL STANDARDS FOR HEALTH CLEARANCE Only required if working on-site at a Partners hospital Description Tuberculosis Screening and Chest X-Rays (One of the following is required) For individuals with a history of a negative TB Test must have documentation of two (2) step TB testing; 1st test within one (1) year of start date, A 2nd test within three (3) months of start date OR Documentation of a negative QFT or Tspot (blood test for TB) within one year of start date B For individuals known to be TB skin test positive or positive QFT or Tspot test, documentation of a chest x-ray which indicates there is no active tuberculosis. Comments: Measles, Mumps, and Rubella Immunity Required (One of the following is required) A Documentation of two measles vaccines, two mumps vaccine, and one rubella (German measles) vaccine or two MMR vaccines. B Proof of immunity via blood test (will show antibodies if immune) to measles, mumps, and rubella (German measles) Comments: Hepatitis B Vaccine1 (For individuals who may be exposed to blood or body fluids) (One of the following is required) A Documentation of three Hepatitis B vaccines B Positive antibody test for hepatitis B Comments: 1 Partners hospital will provide this vaccine free of charge to individuals who may be exposed to blood or body fluid during their work. 2 Verified Partners HealthCare System, Inc. INFECTION CONTROL STANDARDS FOR HEALTH CLEARANCE Only required if working on-site at a Partners hospital Description Verified Chicken Pox (Varicella) Immunity Required (One of the following is required) A Proof of immunity via blood test (will show antibodies if immune) to chicken pox B Documentation of two varicella vaccinations. C Verbal history of chickenpox disease Comments: Tetanus Vaccine Tetanus vaccine within 10 years (Td/Tdap) is strongly recommended but, not required Comments: Influenza Vaccine For All Surgical Technicians & RN Travelers: Seasonal Flu Vaccine required (which can be provided free of charge at the hospital) For all others: Seasonal Flu Vaccine is strongly recommended (which can be provided free of charge at the hospital) Comments: By signing this document the signer attests that the information contain within is accurate and has been obtained legally and with the permission of the stated subject individual. Vendor name: Phone Number: Authorized Signature: Email Address: Printed name: Date: Title: 3