BIE intake form - Spruce Wellness
advertisement

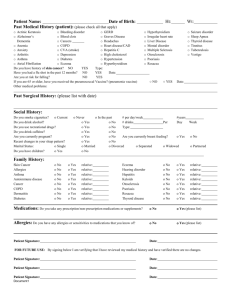
Lifestyle Assessment/Intake Form PART 1 Name: ________________________________ Date of Birth:___________________ Date: ________________ Age:_________________ Sex:______________________ Occupation: _________________________________________________________ What is your purpose for this visit? __________________________________________________________________ What are your main health concerns/complaints? __________________________________________________________________ __________________________________________________________________ Do you have any ailments related to your main health concerns? __________________________________________________________________ What are you current stress levels on a scale of 1 – 10? ____________________________ How does your stress manifest and what are your coping mechanisms? __________________________________________________________________ Are you currently taking any medications or supplements? If so please list. Medication/Supplement Dosage Since Reason What are your favorite foods? _________________________________________________________________ What foods do you crave, if any? ____________________________________________________________ How much water do you consume daily? ____________________________________________________________ Myia Sparreboom RHN/ Spruce Wellness/ www.sprucewellness.ca/ 250-464-4234 Do you experience any symptoms if meals are missed? Explain. __________________________________________________________________ Do you experience any symptoms after eating? Explain. __________________________________________________________________ On a typical day, what do you eat, and at what time: Breakfast:___________________________________________________________ Lunch:_____________________________________________________________ Dinner:____________________________________________________________ Snacks:____________________________________________________________ __________________________________________________________________ Beverages:__________________________________________________________ Are you currently using any other therapies? (naturopathy, exercise, massage, yoga, etc.) Explain.____________________________________________________________ __________________________________________________________________ ________________________________________________ Do you have a support system? (family, friends, church/spiritual practice, etc) __________________________________________________________________ __________________________________________________________________ PART 2 How were you referred? ______________________________________________________________ What problem brings you or your child to this appointment? __________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ What did the symptoms begin? ________________________________________________________ Are your symptoms getting worse? Circle: Yes or No. Do you have any of the following symptoms? Please check all that apply. Cough Wheezing Shortness of Runny Nose Nasal Congestion Itchy Nose Nasal Polyps Poor Sense of Smell Ear Infections Eczema Hives/Swelling Headaches Breath Chest tightness Sneezing Phlegm / Sputum: Itchy / Watery Eyes Postnasal Drip Sinus Infections Blocked Ears Snoring Fatigue Other Color______________ Which of the following trigger (or cause) the symptoms. Please check all that apply. Grass Hay Mold & Mildew Basements Leaves Cats Latex (rubber) Dogs Horses Other animals Alcoholic Beverages Cosmetics Aerosol sprays Other: __________________________ Perfumes Insecticides Odors Drafts House dust Smoke Pollution Exercise Nervousness Cold Air Humidity Weather Changes When are your symptoms worse? Year Round January May September February June October March July November Yes or No. April August December Are symptoms better away from home? Circle: If yes, when? _________________ Occupation (current or previous): ___________________________________________________ Any harmful exposure at work or school? ___________________________________________________ Environmental Survey How long have you lived in your house/apartment? ___________________________________ Approximately how old is your house/apartment/condo? ___________________________________ Do you live in a: House Apt / Duplex Condo / Town House Do you live In the city In the suburbs Rural areas Do you have a basement? Yes No Is your house built on a slab? Yes No Type of heating system? Hot Air Do you use a: Humidifier # Of Pets? Indoor or Outdoor? Steam (radiator) Electric Wood/Coal Stove None Cats Hot water baseboard Dehumidifier Dogs Are there any tobacco smokers in your house? Yes No Is your bedroom in the basement? Yes No Air Cleaner Birds Other Yes Do you have allergy proof encasing for pillow or mattress No What type of pillow do you have? __________________________________________________ What type of comforter do you have? __________________________________________________ What type of floor covering do Wall to wall you have in your bedroom? Area rug Animal skin Bare floor How old is your mattress? ______ What is in your mattress? (I.e. cotton, horsehair, etc.) ___________ Yes Do you have air conditioning? No If yes, Window Unit Do you have problems with roaches or mice? Yes No Do you have water leaks, mold contamination? Yes No Is your home/apartment excessively humid? Yes No Central Your Past Medical History Check all that apply: Diabetes Cancer High blood pressure Anemia/Blood Disorder Asthma Back problems PMS Liver disease/hepatitis Heart problems/murmur Osteoporosis Kidney/bladder Disease Glaucoma Emphysema Endometriosis If yes to any of the above, please explain: Peptic Thyroid disease Arthritis Hay fever Diarrhea Cataracts Infertility Heartburn/reflux Seizures Migraines Depression Anxiety Loss of hearing Menopause ____________________________________________________ ________________________________________________________________________________________ ________________________________________________________________________________________ Have you had your tonsils or adenoids removed? Yes No Have you had ear, nose or sinus surgery? Yes No If yes, please explain: ___________________________________________________________ ___________________________________________________________ Do you smoke now? Yes No How Much? _________________ # Of years? _____ Have you smoked before? Yes No When did you stop? ___________ # Of years? _____ Family History Who in your family has had? Asthma ________________________________________________________________________________ Eczema ________________________________________________________________________________ Seasonal or Year Round Allergies ___________________________________________________________ Other Allergies (drugs/bees/food etc) ________________________________________________________ Sinus Problems _________________________________________________________________________ Please list any hospitalizations regardless of cause: _____________________________________________ ________________________________________________________________________________________ ________________________________________________________________________________________ List any food allergies and reactions experienced: _____________________________________________ ________________________________________________________________________________________ List any drug allergies and reactions experienced (i.e. penicillin, aspirin, sulfa, latex, etc): ______________ ________________________________________________________________________________________ Describe any reaction to insect stings: ____________________________________________________ Food Stressors Section: Check any symptoms that you have experienced: Abdominal cramping Anaphylactic shock Arthritic type symptoms Canker sores Celiac’s disease Constipation Depression Diarrhea or loose stools Difficulty concentrating Emotional upset Eczema Fatigue or sudden drops of energy after meals Gas or bloating Heartburn or indigestion Hives Irritable bowel syndrome (IBS) Irritability Itching – skin or rectal Migraine headaches Nausea Nocturnal enuresis Red rash around mouth, reddening or swelling of skin Rhinitis Runny nose Stiffness of joints Stomach ache Swelling of lips and face Swelling of the joints Vomiting Wheezing Miscellaneous: Indicate any additional information about your symptoms: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ______________________________________ Client Statement I understand and acknowledge that the services hereby provided are at all times restricted to consultation on the subject of health matters intended for general well-being and are not meant for the purposes of medical diagnoses, treatment or prescribing of medicine for any disease, or any licensed or controlled act which may constitute the practice of medicine. This statement is being signed voluntarily. All information will be kept strictly confidential. Name (print):________________________________________________________ Address:____________________________________________________________ __________________________________________________________________ Phone:__________________________ Email:______________________________ Signature:___________________________________ Date:____________________ Thank you. I look forward to working with you. Myia Sparreboom RHN/ Spruce Wellness/ www.sprucewellness.ca/ 250-464-4234