Medical Information
advertisement

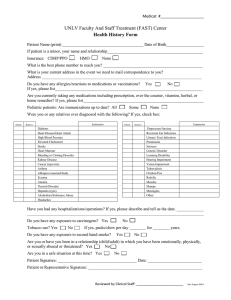
Patient Name: Date of Birth: Past Medical History (patient): (please check all that apply) o Actinic Keratosis o Bleeding disorder o GERD o Alzheimer’s o Blood clots o Graves Disease Dementia o Cancers o Headaches o Anemia o COPD o Heart disease/CAD o Anxiety o CVA (stroke) o Hepatitis C o Arthritis o Depression o High cholesterol o Asthma o Diabetes o Hypertension o Atrial Fibrillation o Eczema o Hyperthyroidism Do you have history of skin cancer? NO YES Type: Have you had a flu shot in the past 12 months? NO YES Date: Are you at risk for falling? NO YES If you are 65 or older, have you received the pneumococcal Vaccine? (pneumonia vaccine) Other medical problems: Ht: o o o o o o o o Wt: o o o o o o Hypothyroidism Irregular heart rate Liver Disease Mental disorder Multiple Sclerosis Otosclerosis Psoriasis Rosacea ○ NO ○ YES Seizure disorder Sleep Apnea Thyroid disease Tinnitus Tuberculosis Vertigo Date: Past Surgical History: (please list with date) Social History: Do you smoke cigarettes? Current Do you drink alcohol? Do you use recreational drugs? Do you drink caffeine? Are you currently pregnant? Recent changes in your sleep pattern? Marital Status: Single Do you have children? Yes Never In the past # per day/week #years Yes No # drinks Per Day Yes No Type: Yes No Yes No Are you currently breast feeding? Yes Yes No Married Divorced Separated Widowed No Week No Partnered Family History: Skin Cancer Allergies Asthma Autoimmune disease Cancer COPD Dermatitis Diabetes No No No No No No No No Yes Yes Yes Yes Yes Yes Yes Yes relative: relative: relative: relative: relative: relative: relative: relative: No No No No No No No No Eczema Hearing disorder Hepatitis Keloids Otosclerosis Psoriasis Rosacea Thyroid disease Yes Yes Yes Yes Yes Yes Yes Yes relative: relative: relative: relative: relative: relative: relative: relative: Medications: Do you take any prescription/non-prescription medications or supplements? No Yes (please list) Allergies: Do you have any allergies or sensitivities to medications that you know of? No Yes (please list) Patient Signature: Date: FOR FUTURE USE: By signing below I am verifying that I have reviewed my medical history and have verified there are no changes. Patient Signature: Date: Patient Signature: Date: Patient Signature: Date: Document1