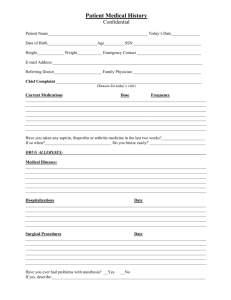
Date of visit: ______ Review of Systems Patient name: Date of birth
advertisement

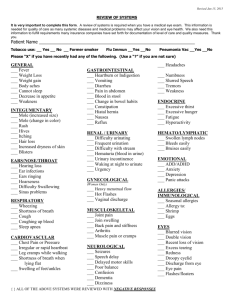
Date of visit: __________ Review of Systems Patient name: ___________________ Date of birth: __________ Are you currently experiencing any of these conditions? Please check all that apply. Constitutional: Cardiovascular: Metabolic/Endocrine: Integumentary: __ Fatigue __ Fever __ Night sweats __ Weakness __ Weight gain __ Weight loss __ Other __________ __ Arrhythmia __ Calf pain __ Chest pressure or discomfort __ Irregular heartbeat/palpitations __ Leg swelling __ Tachycardia __ Other __________ __ Cold intolerance __ Heat intolerance __ Polydipsia __ Polyphagia __ Polyuria __ Other __________ HEENT: Gastrointestinal: __ Exophthalmos __ Hearing loss __ Hoarseness __ Lump in neck __ Nasal congestion __ Sinus problems __ Sore throat __ Tinnitus __ Vertigo __ Other __________ __ Abdominal pain __ Black tarry stools __ Constipation __ Decreased appetite __ Diarrhea __ Dysphagia __ Food intolerance __ Heartburn __ Increased appetite __ Jaundice __ Nausea __ Vomiting __ Other __________ __ Abnormal hair distribution __ Dry skin __ Hives __ Itching skin __ Nail changes __ Rash __ Skin changes __ Skin lesion __ Skin nodules __ Skin sores __ Ulcer __ Other __________ Neurological: Respiratory: __ Asthma __ Cough __ Dyspnea __ Dyspnea on exertion __ Hemoptysis __ Wheezing __ Other __________ Genitourinary: __ Dysuria __ Genital lesions __ Hematuria __ Irregular menses __ Urethral discharge __ Urgency __ Other __________ If none of these symptoms apply check here: N/A ___ __ Balance disturbances __ Dizziness __ Focal weakness __ Gait disturbance __ Headache __ Memory difficulty __ Numbness of extremities __ Other __________ Psychiatric: __ Depressed mood __ Emotional changes __ Euphoria __ Frequent nightmares __ Hallucinations __ Insomnia __ Irritability __ Nervousness __ Stress __ Other __________ Musculoskeletal: __ Arthralgias __ Back pain __ Fracture __ Joint stiffness __ Joint swelling __ Muscle cramping __ Muscle weakness __ Other __________ Hematologic/Lymphatic: __ Bleeding __ Bruising __ Lymphadenopathy __ Tender lymph nodes __ Other __________ Immunologic: __ Environmental allergies __ Food allergies __ Seasonal allergies __ Other __________