Case Study #11: Crohn`s Disease
advertisement

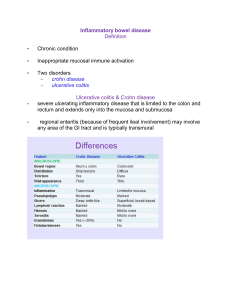
Emily Hawley KNH 411 Case Study #11: Crohn’s Disease 1. What is inflammatory bowel disease? What does current medical literature indicate regarding its etiology? a. Inflammatory bowels disease is an autoimmune, chronic inflammatory condition of the gastrointestinal tract: IBD is actually the term designating a syndrome consisting of two diagnoses: ulcerative colitis and Crohn’s disease. (Nelms 377) The complete etiology of both ulcerative colitis and Crohn’s disease is unknown at the present time, however it is understood that several factors play a role in the conditions. These include environmental considerations such as diet, smoking, infectious agents, physiological changes in the small intestine from which an abnormal inflammatory response is triggered, and intestinal flora. There is a very strong association between genetics and IBS. There is evidence shows that with a positive family history, 5-15% of patients will have IBS. Identical twins there is a 44% chance and fraternal a 3.8% chance (415). Several tests can be done in order to diagnose inflammatory bowel disease. These include abdominal ultrasound, MRI, CT scan, and antiglycan antibodies. The most prevalent way to diagnose and describe Crohn’s disease is using the CDAI. A score of over 150 indicates a flare-up of the disease, and a score over 300 means the patient is experiencing a severe exacerbation of the disease. Calprotectin, lactoferrin, and polymorphonucler nuetrophil electase levels in the stool have been found to be indicative of exacerbations of Crohn’s disease as well. Low albumin levels and elevated WBC are also common. In the case of ulcerative colitis, more than 5 daily bowel movements, large amounts of hematochezia, temperature above 37.5°C, pulse above or equal to 90/min, and hemoglobin less than 10 g/dL are all indicative of severe activity of ulcerative colitis (416). 2. Mr. Sims was initially diagnosed with ulcerative colitis and then diagnosed with Crohn’s. How could this happen? What are the similarities and differences between Crohn’s Disease and ulcerative colitis? Mr. Sims ulcerative colitis could have gotten worse and been considered Crohn’s because of the further infected GI mucosa. UC and Crohn’s are both characterized by exacerbations of the disease process interspersed with period of remission. 50% of patients with UC have the disease only involving the rectum. Damage to the intestinal mucosa only involves the first two layers of tissues in the colon and rectum. Crohn’s disease can affect any portion of the GI tract from the mouth to the anus, but mostly affects the ileum and colon. Crohn’s disease can damage all layers of the GI mucosa (417). 3. A CT scan indicated bowel obstruction and the Crohn’s Disease was classified as severe-fulminant disease. CDAI score of 400. What does a CDAI score of 400 indicate? What does a classification of severefulminant disease indicate? CDAI score of 400 falls into the Moderate-Severe Disease being between 220 and 450. This means that the individuals who have failed to respond to treatment for the stage below or patients with more major symptoms including fevers, significant weight loss, abdominal pain or tenderness, intermittent nausea or vomiting, or significant anemia. Severe-fulminant disease indicates that individuals have persisting symptoms even with introduction to steroids or biologic agents as outpatients, or they have high fevers, persistent vomiting, evidence of intestinal obstruction, rebound tenderness, cachexia, or evidence of abscess (419). 4. What did you find in Mr. Sims’ history and physical that is consistant with his diagnosis of Crohn’s? Explain. Mr. Sims is running a fever of 101.5. His abdomen is distended and there is extreme tenderness which is causing him extreme abdominal pain and cramping. There is minimal bowel sounds. He is experiencing more chronic diarrhea as he stated he is experiencing it more often. Patient is constantly losing weight. He was first diagnosed with ulcerative colitis which later turned into Crohn’s after it become more severe. 5. Crohn’s patients often have extraintestinal symptoms of the disease. What are some examples of these symptoms? Is there evidence of these in his history and physical? Extraintestinal symptoms of Crohn’s disease are symptoms that happen outside of the GI tract. These symptoms include osteopenia and osteoporosis, dermatitis, rheumatological conditions such as ankylosing spondylitis, ocular symptoms, and hepatobiliary complications (418). Mr. Sims is not experiencing any of these symptoms in his history or physical. 6. Mr. Sims has been treated previously with corticosteroids and mesalamine. His physician had planned to start Humira prior to his admission. Explain the mechanism for each of these medications in the treatment of Crohn’s. Treatments for inflammatory bowel syndrome include antibiotics, immunosuppressive medications, immunomodulators, and biologic therapies as well as surgical intervention. Corticosteroids like presnisone or budenoside are often used to treat acute exacerbations, especially in severe-fulminant disease, but patients are at risk for becoming steroid dependant. Aminoalicylate medications like mesalamine and sulfasalazine are used in Crohn’s disease when the ileal and colon are involved. Antibiotics and biological therapies such as antiadhesion molecules and anti-interleukin antibodies are also used. Humira is a biologic therapy for Crohn’s disease, which works to interrupt tumor necrosis factor alpha and thus the cytokinedirected inflammatory activity (419). 7. Which laboratory values are consistent with an exacerbation of his Crohn’s disease? Identify and explain these values. Mr. Sims has decreased protein, Albumin, and Prealbumin levels. Protein values need to be increased because a lot of it is lost due to the inflammation of the GI tract. ASCA, which is the presence of antibodies, is high which is specific to Crohn’s. Hematocrit is low, Hemoglobin is low, transferrin is low, ferritin Is low due to blood loss and malabsorption. Vitamin D and free retinol(Vitamin A) is lost through steatorrhea (420). 8. Mr. Sims is currently on several vitamin and mineral supplements. Explain why he may be at risk for vitamin and mineral deficiencies. Mr. Sims is at risk for vitamin and mineral deficiencies because t is common to have nutrient deficiencies with Crohn’s disease. Protein-calorie malnutrition as well as other nutrient deficiencies can be caused by decreased nutrient intake, malabsorption, drug-nutrient interactions, anorexia, and protein losing enteropathy. Without taking supplements it can lead to osteoporosis, anemia, poor wound healing, and a compromised immune system. Increased motility decreases the success of digestion and absorption, severe diarrhea can result in malabsorption of all nutrients. A lot of the time patients reduce intake to decrease their symptoms which further decreases dietary intake (420). 9. Is Mr. Sims likely a candidate for short bowel syndrome? Define short bowel syndrome, and provide a rationale for your answer. Short bowel syndrome results from a large resection of the small intestine. Since Mr. Sims is a candidate for short bowel syndrome because he has a disease associated with loss of absorption and is characterized by the inability to maintain protein, energy, fluid, electrolyte, and micronutrient balance when on a conventionally accepted, normal diet (424). 10. What type of adaption can the small intestine make after resection? There are three phases for SBS post operation. The first stage involves extensive fluid and electrolyte loss with large volumes of diarrhea. The second phase involves the reduction of diarrhea volumes for several months. During the third phase, there is continued adaptation of the remaining bowel. That includes increased blood flow, secretions, and mucosal cell growth. The inner lumen of the small intestine increases both in length and diameter with additional increase in villous height. This phase lasts for 1 or 2 years (425). 11. For what classic symptoms of short bowel syndrome should Mr. Sims’ health care team monitor? Short bowel syndrome is characterized by inability to maintain protein, energy, fluid, electrolytes, or micronutrient balances on a normal diet (424). 12. Mr. Sims is being evaluated for participation in a clinical trial using high-dose immunosuppression and autologous peripheral blood stem cell transplantation. How might this treatment help Mr. Sims? Most transplants are done by peripheral blood tem cell transplantations. This will help Mr. Sims because it is a different route to go for treatment since he does keep getting worse every time he goes into the hospital. Delayed gastric emptying may persist for months following the transplant, which would help Mr. Sims, gain weight (717). 13. What are the potential nutritional consequences of Crohn’s Disease? Potential nutritional consequences of Crohn’s Disease includes: cachexia, which is body emaciation by the fat and muscles catabolizing to fuel the inflammatory response; Vitamin deficiency due to the malabsorption of essential nutrients; Parenteral Nutrition due to the incapability of absorbing essential nutrients; and malabsorption of fat due to the rapid passing through diarrhea (crohn). 14. Mr. Sims underwent resection of 200 cm of jejunum and proximal ileum with placement of jejunostomy. The ileocecal valve was preserved. Mr. Sims did not have an ileostomy, and his entire colon remains intact. How long is the small intestine and how significant is this resection? The small intestine is about 6 meters, or 20 feet long. 200 cm is equal to 2 meters in length so the resection removed about 1/3 of the small intestine, which would make the resection very significant. 15. What nutrients are normally digested and absorbed in the portion of the small intestine that has been resected? Jejunum is responsible for absorption of lipophilic nutrients (proteins, fats, cholesterol and the fat-soluble vitamins A, D, E and K) and absorption of water. The ileum is the primary site of reabsorption of bile acids, B12, and anything the jejunum didn’t absorb. 16. Evaluate Mr. Sims’ % UBW and BMI. %UBW= (100 x Actual Weight)/Usual body weight =(100 x 140)/167 =83.8% BMI= 63.5 kg/ 1.752 =20.8 17. Calculate Mr. Sims’ energy requirements. Harris Benedict= 66.5+(13.75 x 63.5)+(5 x 175)-(6.78 x 35) =1,577.3 EER= 1,577.3 x 1.6 = 2,523.7 *Increase energy requirements for healing process to 2,800 18. What would you estimate Mr. Sims’ protein requirements to be? Protein requirements= weight in kg x 1.5 g/kg 63.5 kg x 1.5g/kg= 95.3 g/day PRO Protein requirement increased to 1.5g/kg for adults with GI inflammation 19. Identify any significant and/or abnormal laboratory measurements from both his hematology and his chemistry labs. Chemistry Protein Deficient by 0.5 g/dL Albumin Deficient by 0.3 g/dL Prealbumin Deficient by 5.0 mg/dL HDL Low by 7 mg/dL Hematology Hemoglobin Low 1.1 g/dL Hematocrit Deficient by 2% Transferrin Low by 35 mg/dL Ferritin Low by 4 mg/mL Vitamin D Deficient by 7.3 ng/mL Vitamin A Deficient by 2.8 ug/dL 20. Select two nutrition problems and complete the PES statement for each. (NC-3.2) Involuntary weight loss related to abdominal pain and admission to hospital for Crohn’s flare as evidenced by significant weight loss. (NC-1.4) Altered GI function related to abdominal pain, tenderness, and diarrhea as evidenced by history of Crohn’s disease. 21. The surgeon notes Mr. Sims probably will not resume eating by mouth for at least 7-10 days. What information would the nutrition support team evaluate in deciding the route for nutrition support? Seven things in developing the PN prescription is: A. Establish dosing weight and energy requirements B. Calculate a protein goal C. Distribute remaining kcal between carbohydrate and lipid D. Consider the electrolyte needs for this patient E. Consider vitamin and mineral requirements F. Establish fluid requirements G. Calculate the final parenteral prescription (97). 22. The members of the nutrition support team note his serum phosphorus and serum magnesium are at the low end of the normal range. Why might that be of concern? It is critical to monitor serum levels of phosphorus, magnesium, and potassium, and to provide supplementation as needed until the patient is receiving goal feedings. It needs to be monitored to avoid overfeeding and avoid refeeding syndrome. Low levels may result in hemolysis, impaired cardiac function, impaired respiratory function, and even death (93). 23. What is refeeding syndrome? Is Mr. Sims at risk for this syndrome? How can it be prevented? Refeeding syndrome is a term used to describe several common metabolic alterations that may occur during nutritional repletion of starved patients. It is a risk for patients who present with malnutrition, those who have a history of long term inadequate oral intake, and those who have had minimal intake for several days as a result of NPO status or poor appetite (92). 24. Mr. Sims was placed on parenteral nutrition support immediately postoperatively, and a nutrition support consult was ordered. Initially, he was prescribed to receive 200 g dextrose/L, 42.5 g amino acids/L, and 30 g lipid/L. His parenteral nutrition was initiated at 50cc/hr with a goal rate of 85 cc/hr. Do you agree with the team’s decision to initiate parenteral nutrition? Will this meet his estimated nutritional needs? Explain. Calculate: pro (g); CHO (g); lipid (g); and total kcal from his PN. PN is a good decision because he is unable to meet his nutritional needs either by an oral diet or through use of enteral nutrition. He will better absorb nutrients after his bowel resection (93). PRO (g): 2,523.7/4= 630.9(30%)= 189 g CHO (g): 2,523.7/4= 630.9(50%)=315.5 g Lipid (g): 2,523.7/9=280.4(20%)= 56.1 Total kcal: 2,523.7 kcal 25. For each of the PES statements you have written, establish an ideal goal (based on the signs and symptoms) and an appropriate intervention (based on the etiology). A few goals based off of the PES statements are to increase his weight, increase physical activity and normalize his GI function. After Mr. Sims is discharged from the hospital a nutrition consult will be done to discuss ways to increase his weight and send him home with a few menu ideas. The dietitian will discuss the importance of a higher protein diet (150% above normal protein requirements) and the importance of fat content as well. Another goal is to normalize his GI tract and decrease his diarrhea Dietary fiber intake may improve symptoms of patients with inflammatory bowel disease. 26. Indirect calorimetry revealed the following information: Measure Mr. Sims’ Data Oxygen Consumption (mL/min) 295 CO2 production (mL/min) 261 RQ 0.88 RMR 2022 What does this information tell you about Mr. Sims’? Indirect calorimetry is used to determine the energy requirements of critically ill or mechanically ventilated patients, and to monitor the adequacy and appropriateness of nutritional support. Mr. Sims is burning a lot of his calories while at rest. 27. Would you make any changes to his prescribed nutrition support? What should be monitored to ensure adequacy of his nutrition support? Explain. I would increase his energy needs due to the fact that at his resting metabolic rate he is burning a high amount of energy. 28. What should the nutrition support team monitor daily? What should be monitored weekly? Explain your answers. The patient can also receive many infections while on the PN. An infection can be introduced into the bloodstream as well as the GI tract because it is non-functioning. The risk for infection should be monitored daily (101). The patients weight should be monitored weekly because there will be involuntary weight loss during the tube feeding. Oral diet is the best way to achieve nutrition goals and without it the patient can lose weight (102). 29. Mr. Sims’ serum glucose increased to 145 mg/dL. Why do you think this level is now abnormal? What should be done about it? This means that his blood glucose levels are high. This level is now abnormal because the PN has too high of a carbohydrate content. The dextrose levels in the PN order should be decreased to lower hi serum glucose to a normal range below 125 mg/dL. 30. Evaluate the following 24 hour urine data: 24 hour urinary nitrogen for 12/20:18.4 grams. By using the daily input/output record for 12/20 that records the amount of PN received, calculate Mr. Sims’ nitrogen balance on postoperative day 4. How would you interpret this information? Should you be concerned? Are there problems with the accuracy of nitrogen balance studies? Explain. Urinary nitrogen test is used primarily as a biomarker of the validity of dietary assessments; 24-hour urine nitrogen is the most well known biological marker. The apparent accuracy of 24-hour urine nitrogen as a biological marker led to the suggestion that it be used to validate estimates of protein intake from various dietary survey methods. The use of 24-hour urine nitrogen depends on the assumption that subjects are in nitrogen balance and there is no accumulation due to growth or repair of lost muscle tissue or loss due to starvation, dieting or injury. (Bingham) 31. On post op day 10, Mr. Sims’ team notes he has had bowel sounds for the previous 48 hours and had his first bowel movement. The nutrition support team recommends consideration of an oral diet. What should Mr. Sims be allowed to try first? What would you monitor for tolerance? If successful, when can the parenteral nutrition be weaned? A liquid diet ensures that the area around the removed parts of the GI tract begin to heal properly without disruption possible irritating food particles. Within a few days a soft diet will begin. If the soft diet seems to work then he can slowly start to come back to a normal diet again with the restrictions of the diet he was already on to prevent another surgery. 32. What would be the primary nutrition concerns as Mr. Sims prepares for rehabilitation after his discharge? Be sure to address his need for supplementation of any vitamins and minerals. Identify two nutritional outcomes with specific measures for evaluation. His primary nutrition concerns as he prepares for discharge is to be sure to obtain enough energy and protein needs. He should eat smaller meals more often and be sure that he chews his food well. Separate solids and liquids during the meal as much as possible because too much liquid can cause a column effect. Avoid stimulants like alcohol and caffeine as much as possible. Vitamins and minerals are very important due to the fact there will be less absorption in the GI tract so supplementation will be needed. Foods high in these have been associated with protection against inflammation. Two outcomes will be weight gain to his usual body weight of 166-168 lbs. as well as reduce his inflammation down by taking supplements with probiotics and prebiotics to be able to eat a normal diet (422.) References Bingham, S. (2003) Urine Nitrogen as a Biomarker for the Validation of Dietary Protein Intake. Journal of Nutrition.