Sample Form - The Wistar Institute
advertisement

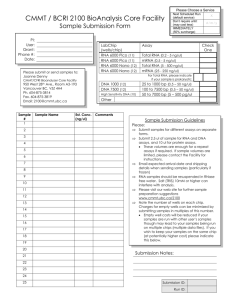
Genomics Core Facility Sample DNA/RNA Form The Wistar Institute Louise Showe Date: lshowe@wistar.org Room 372E OVQ 380 S. University Avenue Philadelphia PA 19104 215-898-3902 Wistar_____ External_____ Adjunct_____ Name (P.I. and Sample Provider): Address: City, State, Zip Code: Email: Billing Information: Contact: Address: Email: Grant/PO number: Phone: Phone: Please answer the following questions and provide the specified documents listed below: Note: Please also provide all information clearly on the DNA/RNA sample tubes. 1. Species of isolated DNA/RNA 2. Number of samples 3. Stored at 4. RNA Sample (check one) ___Total RNA ___DNAse treated Total RNA 5. Concentration of DNA/RNA (ng/ul, pg/ul) Total volume (ul) 6. Please provide a gel image of all DNA/RNA samples 7. One Paragraph summary of Project 8. Comments/Specific Instructions: Please contact Bioinformatics Facility (bioinfo@wistar.org) for data analysis