March 2014 - Piriformis Syndrome
advertisement

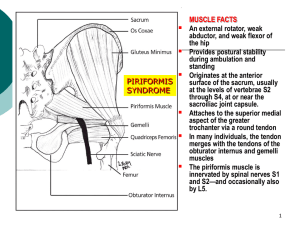
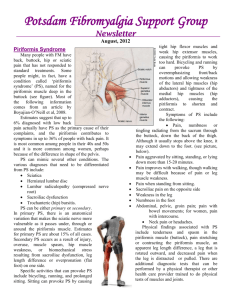
Journal Club March 2014 Brought to you by the AOCPMR Student Council Article title: Brief review: Piriformis syndrome; etiology, diagnosis, and management Authors: Danilo Jankovic MD, Philip Peng MBBS, Andre van Zundert MD PhD Journal/Source: Can J Anesth/J Can Anesth (2013) 60:1003-10012 Discussion: This review article focused on providing a well rounded looks at piriformis syndrome; including etiology diagnosis and management. The principal source of data was collected using a literature search of the MEDLINE® database from January 1980 to December 2012. Conservative estimates of new cases of lower back pain and sciatica total 40 million annually and with piriformis syndrome responsible for 5-6% of cases of sciatica, this topic would represent an incidence of 2.4 million per year. Many etiological factors may account for the symptoms of piriformis syndrome, however in most patients there is no identifiable cause. Clinical presentation is mainly divided into somatic and neuropathic components. The somatic component is a myofascial pain syndrome, and the neuropathic component refers to the compression or irritation of the sciatic nerve as it courses through the infrapirifom foramen. There is no gold standard in diagnosing piriformis syndrome. The physical exam is important in revealing well-described signs such as piriformis, Freiberg’s, Pace’s, and Lasegue’s signs. Beatty’s maneuver as well as the Hughes test may also be positive. Electrophysiological tests serve as a means of diagnosis if the muscle is stressed as with the FAIR test. Other diagnostic imaging modalities include CT, MRI, scintigraphy, and ultrasound. Piriformis syndrome typically responds to conservative treatments such as physical therapy, lifestyle modifications, psychotherapy and pharmacological agents such as NSAIDs, muscle relaxants and neuropathic pain medications. Surgical treatment is seldom necessary. 1 www.aocpmr.org Current techniques in piriformis muscle injection are offered to patients as part of a multimodal therapy. An ultrasound-guided injection has the advantage over the CT-guided technique in that it avoids radiation exposure, offers real-time surveillance of the injection, and is more affordable. The accuracy of needle placement with ultrasound was validated with accuracy suggestive of 95%. Injections of local anesthetics, steroids, and botulinum toxin into the piriformis muscle can serve both diagnostic and therapeutic purposes. In order to optimize management of piriformis syndrome an interdisciplinary evaluation of treatment should be utilized. Questions: 1) Discuss the anatomical variation as well and their impact on diagnosis and treatment of piriformis syndrome. 2) With no gold standard in diagnosis, under what circumstances and with which modality would you evaluate someone for piriformis syndrome? 3) Discuss the role of OMM in the treatment of piriformis syndrome regarding the somatic and neuropathic components. Reviewer: Gary Panagiotakis, OMS-IV, AOCPMR Student Council Education Committee 2 www.aocpmr.org