Lower Extremity Orthoses: Types, Indications & Use
advertisement

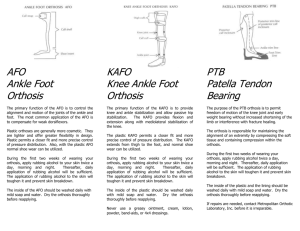
Corrective lower extremity Orthoses A lower limb Orthosis, is an external device applied or attached to a lower body segment to improve function by controlling motion, providing support through stabilizing gait, reducing pain through transferring load to another area, correcting flexible deformities, and preventing progression of fixed deformities California Biomechanics Laboratory Orthotics (UCBL) Figure 1 UCBL There are three main corrective forces found in a UCBL foot orthotic. A deep, well moulded, heel cup that holds the hind foot in the corrected position while the arch of the UCBL supports the mid foot, stabilizing the midtarsal joint, and the lateral wall controls the outside border of the foot. Indications Adult acquired flatfoot Posterior tibial tendon dysfunction Flexible pes planus Plantar fasciitis Heel Spurs Flexible metatarsus adductus/abductus Midfoot fracture Gait Plates for in toeing or out toeing Figure 2 Gait plate In-toeing means that when a child walks or runs, the feet turn inward instead of pointing straight ahead. It is commonly referred to as being "pigeon-toed." In-toeing is often first noticed by parents when a baby begins walking, but children at various ages may display in-toeing for different reasons. Occasionally, severe in-toeing may cause young children to stumble or trip as they catch their toes on the other heel. In-toeing usually does not cause pain, nor does it lead to arthritis. In the vast majority of children younger than 8 years old, in-toeing will almost always correct itself without the use of casts, braces, surgery, or any special treatment. Causes of in-toeing The cause of in-toeing depends on where the change in alignment is centred. There are three common conditions causing in-toeing: Curved foot (metatarsus adductus) – Orthotic treatment proved successful Twisted shin (tibia torsion) - Splints, special shoes, and exercise programs not proven to help Twisted thighbone (femoral anteversion) - Splints, special shoes, and exercise programs not proven to help Each of these conditions may run in families. They also can simply occur on their own or in association with other orthopaedic problems. Prevention is not usually possible because they occur from developmental or genetic problems that cannot be controlled for. Out-toeing is much less common than in-toeing. The most typical presentation is within the first or second year of life. Most children are born with external rotation contractures of the hips and this resolves shortly after walking begins. In those children in whom the resolution is slower, out-toeing is the result when they first start walking. This will almost always resolve within a year from the onset of walking. Gait plate Gait Plates work by utilizing a semi-rigid shell that effectively alters the break of the ball of the foot during propulsion to encourage realignment of the hip in gait. Gait Plates further address foot pronation which is typically associated with childhood gait abnormalities by incorporating the features of a functional foot orthosis (i.e. deep heel cup, medial rear foot posting and skive) to control subtalar joint pronation during contact and mid-stance phases of gait. Out Toe Gait Plate: Induces an improved outward position of the foot. Out-Toe Plate has lateral flange and lateral extension of the distal edge extending under the fifth metatarsal head to the sulcus. In Toe Gait Plate: Induces an improved inward position of the foot. In-Toe Plate has medial flange or distal extension under the first metatarsal head. Ankle Foot Orthosis (AFO) AFO's are generally prescribed to control spasticity in children with Cerebral Palsy, drop foot for children with hemiplegia or children with low tone and hyper-mobility of the foot and ankle joints. Custom made from casts, AFO's are designed to maintain foot and ankle positioning or reduce the effects of spasticity. AFO's assist children to stand, walk or play more naturally or efficiently. Supra Malleolar Orthosis (SMO) The SMO, as with other orthoses, gets its name for the part of the body for which it encompasses. This orthosis supports the leg just above the malleoli. The SMO is considered the shortest of the Ankle Foot Orthoses or AFO's. It gets prescribed for patients who have soft, flexible, flat feet. SMO’s are often worn by children. The medical term for a flat foot is a pronated foot or pes planus, pes plano-valgus, and hyper-pronated foot. The SMO is designed to maintain a vertical, or neutral heel while also supporting the three arches of the foot. This can help improve standing balance and walking. Hind foot Control Orthosis Recommended for: Significant forefoot, mid-foot, and subtalar instability Global foot deviations due to low or high tone Foot deviations that interfere with stance and balance Young children with significant foot instability that need free dorsiflexion and plantarflexion for crawling, pulling to stand, and squatting Not recommended for: Knee flexion or extension instability Persistent toe walking Dynamic Ankle Foot Orthosis (DAFO) Figure 3 Dynamic AFO The DAFO is designed to stabilise the foot in the mediolateral plane, and to help the child maintain a functional position, to improve stability for successful standing and walking. It also gives excellent proprioceptive feedback from the ground using a dynamic foot plate. The DAFO differs from a traditional AFO which is typically stiff and rigid, by being, flexible and wraps around the patient’s entire foot in order to provide improved sensation and alignment. Initially it was designed for use by paediatric patients but is now sometimes used by the adult patients as well, a DAFO encourages range of motion, allowing children to learn movement by moving and providing minimal support, only where the patient needs it. DAFOs are frequently prescribed to assist with mobility and motor skills of children with cerebral palsy, spina bifida, muscular dystrophy, clubfoot and autism. The concept for the original DAFO was developed in 1985 as collaboration between Don Buethorn, CPO, and Nancy M. Hylton, PT, LO. The two worked together to create a thin, flexible brace that would meet the needs of paediatric patients with neurodevelopment challenges. Ankle Foot Orthosis, Fixed and Hinged (AFO) AFOs come in many different specifications and are custom made. We can design them to be fixed at the ankle; this allows us to fine tune the gait more effectively. Or they can hinge at the ankle to allow limited range of movement in one plane. Figure 4 Leaf spring and articulating AFO Knee Ankle Foot Orthosis (KAFO) A knee-ankle-foot orthosis (KAFO) is an orthosis that encumbers the knee, ankle and foot. Motion at all three of these lower limb areas is affected by a KAFO and can include stopping motion, limiting motion, or assisting motion in any or all of the 3 planes of motion in a human joint: saggital, coronal, and axial. The selection process of the correct KAFO is quite involved, and both the materials and the functions which the orthosis is intended to fulfil play a decisive role. With modern materials, only the functionally relevant body regions have to be surrounded and supported. Hip Knee Ankle foot Orthosis(HKAFO) The HKAFO is a KAFO (knee-ankle-foot-orthosis) with an extension of hip joint and pelvic devices. This orthotic is used for patients/clients requiring extra stability of the hip due to paralysis and weakness that also accompany lower extremity involvement. The HKFO brace will provide pelvic stability in all planes of movement. The hip joint of the brace stabilizes and aligns the lower leg, which reduces undesired motion and increases steps per minute and reduces energy output. Just as eyeglasses do not change a person’s eye but help prevent further eye problems, a pair of orthotics will prevent further damage and slow down the progression of the pathology. Orthotics will compensate for problems and allow a child to exercise or participate in normal daily activities more comfortably and preventing secondary damage.