IEP Audit and Transfer of Records - 2014
advertisement

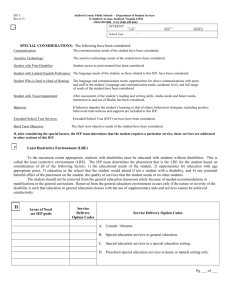
Student Names Case Manager _____________________ *** Copies to Receiving School and EC Department*** Receiving EC Teacher’s Signature ___________________ Date ______________ IEP Chair signature___________________________ Date______________ Report(s) of Progress OT/PT/SLP Related Services Support( if applicable) Secondary Transition component (14 +) Copy given/sent to Parent(s) Record of IEP Participation ESY (Addressed on IEP ,worksheet included and addendum if needed) LRE Justification Statement Continuum of Alternative Educational Placements Nonacademic Services & Activities Frequency and Location of Related Services Frequency and Location of Special Ed Alternate Assessment Justification District-Wide Assessment Program NC Assessment Program Technical Assistance addressed Implementation Specifications in regular program Aids, services, modification in regular program LRE/General Education Program participation Description of how Annual Goal will be measured Criteria for Mastery specified for Benchmarks and Short Term Objectives Benchmarks or Short Term Objectives Measurable Annual Goals (academic or functional) Assistive technology and integration with related services addressed Competency Goal–based on NCSCOS (n/a for Extend 1 students) Present Level of Academic & Functional Performance (directly related to goals) Consideration of Special Factors (attachment HI only) Consideration of Transitions Student Profile Area(s) of Eligibility Current Reevaluation Due Date DEC 6 (Consent for Placement) VANCE COUNTY SCHOOLS Department for Exceptional Children INDIVIDUAL EDUCATION PLAN AUDIT and TRANSFER OF RECORDS FORM Principal’s signature__________________________ Date_______________ Comments: ___________________________________________________________________________________